

Tobacco smoking and risks of more than 470 diseases in China: a prospective cohort study
- PMID: 36462513
- PMCID: PMC7613927
- DOI: 10.1016/S2468-2667(22)00227-4
Tobacco smoking and risks of more than 470 diseases in China: a prospective cohort study
Abstract
Background: Tobacco smoking is estimated to account for more than 1 million annual deaths in China, and the epidemic continues to increase in men. Large nationwide prospective studies linked to different health records can help to periodically assess disease burden attributed to smoking. We aimed to examine associations of smoking with incidence of and mortality from an extensive range of diseases in China.
Methods: We analysed data from the prospective China Kadoorie Biobank, which recruited 512 726 adults aged 30-79 years, of whom 210 201 were men and 302 525 were women. Participants who had no major disabilities were identified through local residential records in 100-150 administrative units, which were randomly selected by use of multistage cluster sampling, from each of the ten diverse study areas of China. They were invited and recruited between June 25, 2004, and July 15, 2008. Upon study entry, trained health workers administered a questionnaire assessing detailed smoking behaviours and other key characteristics (eg, sociodemographics, lifestyle, and medical history). Participants were followed up via electronic record linkages to death and disease registries and health insurance databases, from baseline to Jan 1, 2018. During a median 11-year follow-up (IQR 10-12), 285 542 (55·7%) participants were ever hospitalised, 48 869 (9·5%) died, and 5252 (1·0%) were lost to follow-up during the age-at-risk of 35-84 years. Cox regression yielded hazard ratios (HRs) associating smoking with disease incidence and mortality, adjusting for multiple testing.
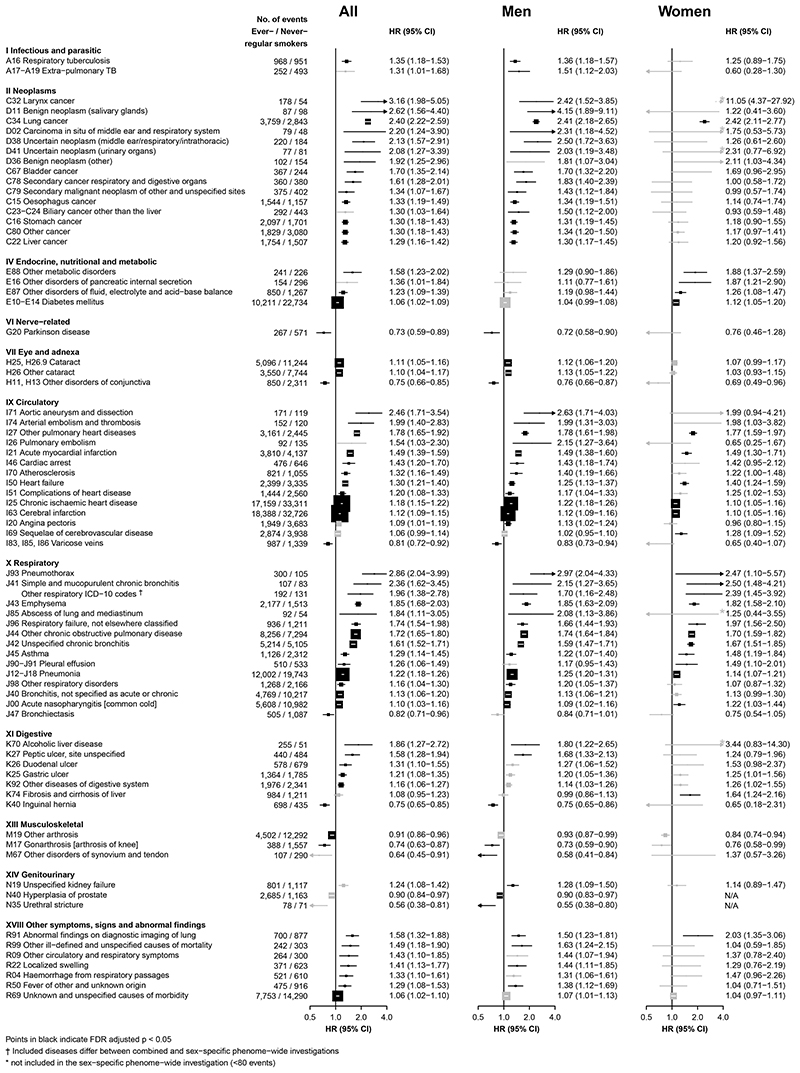
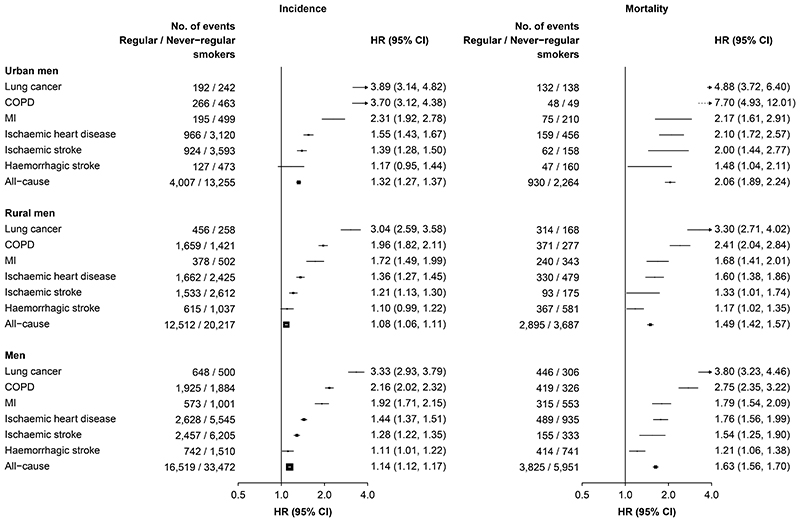
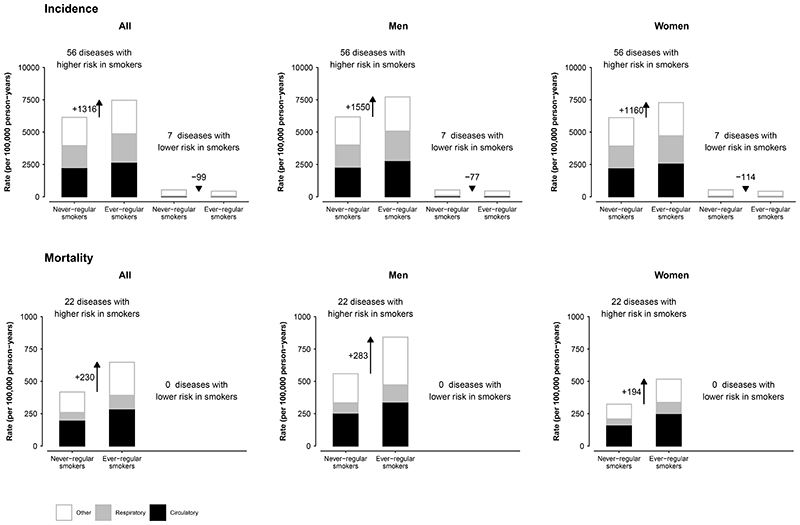
Findings: At baseline, 74·3% of men and 3·2% of women (overall 32·4%) ever smoked regularly. During follow-up, 1 137 603 International Classification of Diseases, 10th revision (ICD-10)-coded incident events occurred, involving 476 distinct conditions and 85 causes of death, each with at least 100 cases. Compared with never-regular smokers, ever-regular smokers had significantly higher risks for nine of 18 ICD-10 chapters examined at age-at-risk of 35-84 years. For individual conditions, smokers had significantly higher risks of 56 diseases (50 for men and 24 for women) and 22 causes of death (17 for men and nine for women). Among men, ever-regular smokers had an HR of 1·09 (95% CI 1·08-1·11) for any disease incidence when compared with never-regular smokers, and significantly more episodes and longer duration of hospitalisation, particularly those due to cancer and respiratory diseases. For overall mortality, the HRs were greater in men from urban areas than in men from rural areas (1·50 [1·42-1·58] vs 1·25 [1·20-1·30]). Among men from urban areas who began smoking at younger than 18 years, the HRs were 2·06 (1·89-2·24) for overall mortality and 1·32 (1·27-1·37) for any disease incidence. In this population, 19·6% of male (24·3% of men residing in urban settings and 16·2% of men residing in rural settings) and 2·8% of female deaths were attributed to ever-regular smoking.
Interpretation: Among Chinese adults, smoking was associated with higher risks of morbidity and mortality from a wide range of diseases. Among men, the future smoking-attributed disease burden will increase further, highlighting a pressing need for reducing consumption through widespread cessation and uptake prevention.
Funding: British Heart Foundation, Cancer Research UK, Chinese Ministry of Science and Technology, Kadoorie Charitable Foundation, UK Medical Research Council, National Natural Science Foundation of China, Wellcome Trust.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
References
-
- Eriksen M, Mackay J, Schluger N, Gomeshtapeh FI, Drope J. The Tobacco Atlast. 5th. American Cancer Society; Atlanta, Gerogia 30303, USA: 2015. Smoking Among Women.
-
- Chinese Center for Disease Control and Prevention. China Adult Tobacco Survey Report 2018: Chinese Center for Disease Control and Prevention, 2019
-
- Doll R, Peto R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J Natl Cancer Inst. 1981;66(6):1191–308. - PubMed
-
- Wald N, Nicolaides-Bouman A. UK Smoking Statistics. 1991
-
- US Department of Health and Human Services. The health consequences of smoking - 50 years of progress: a report of the Surgeon General. US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; Atlanta, GA, US: 2014.
Publication types
MeSH terms
Grants and funding
- MC_U137686851/MRC_/Medical Research Council/United Kingdom
- 29186/CRUK_/Cancer Research UK/United Kingdom
- RE/18/3/34214/BHF_/British Heart Foundation/United Kingdom
- C16077/ A29186 /CRUK_/Cancer Research UK/United Kingdom
- MC_UU_00017/1/MRC_/Medical Research Council/United Kingdom
- CH/1996001/9454/BHF_/British Heart Foundation/United Kingdom
- MC_PC_12027/MRC_/Medical Research Council/United Kingdom
- MC_UU_12026/2/MRC_/Medical Research Council/United Kingdom
- 202922/WT_/Wellcome Trust/United Kingdom
- A16896/CRUK_/Cancer Research UK/United Kingdom
- MC_EX_G0801669/MRC_/Medical Research Council/United Kingdom
- 212946/WT_/Wellcome Trust/United Kingdom
- MC_U137686854/MRC_/Medical Research Council/United Kingdom
- MC_PC_12029/MRC_/Medical Research Council/United Kingdom
- G0300622/MRC_/Medical Research Council/United Kingdom
- MC_PC_12028/MRC_/Medical Research Council/United Kingdom
- 088158/WT_/Wellcome Trust/United Kingdom
- 104085/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
