

A randomized clinical trial of isolated ambulatory phlebectomy versus saphenous thermal ablation with concomitant phlebectomy (SAPTAP Trial)
- PMID: 36464887
- PMCID: PMC10364515
- DOI: 10.1093/bjs/znac388
A randomized clinical trial of isolated ambulatory phlebectomy versus saphenous thermal ablation with concomitant phlebectomy (SAPTAP Trial)
Abstract
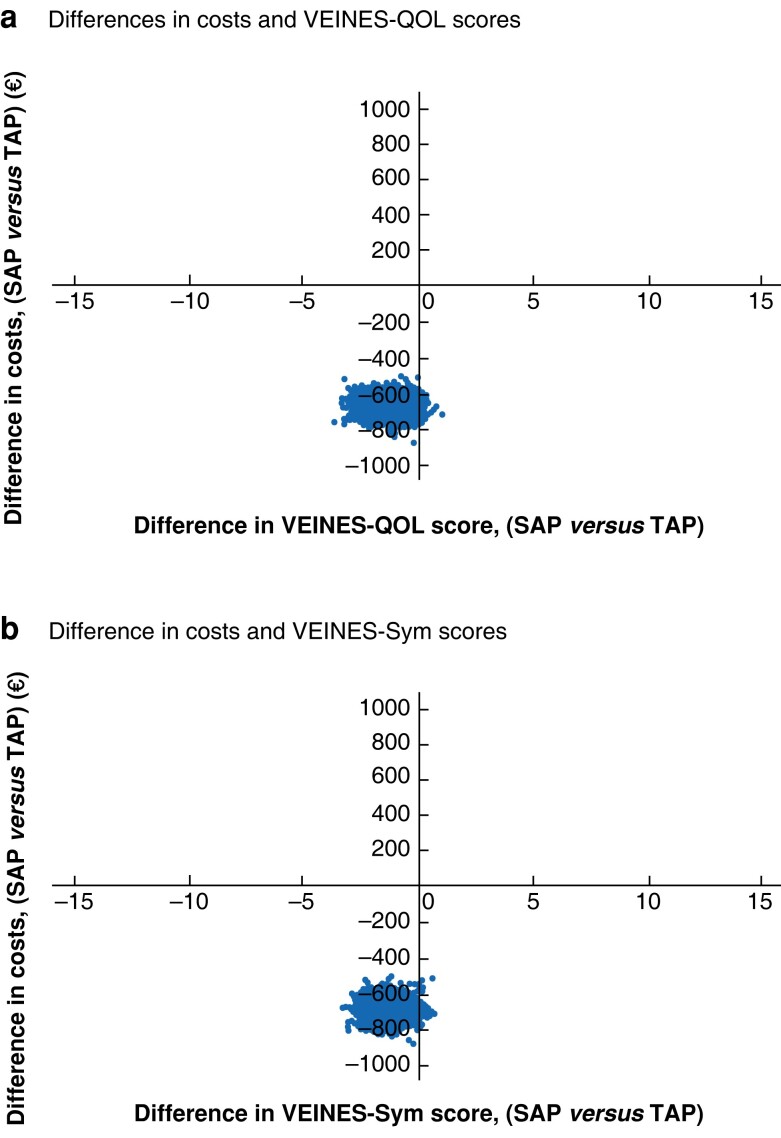
Background: Current treatment of patients with saphenous trunk and tributary incompetence consists of truncal ablation with concomitant, delayed or no treatment of the tributary. However, reflux of the saphenous trunk may be reversible after treatment of the incompetent tributary. The aim of this study was to determine whether single ambulatory phlebectomy with or without delayed endovenous truncal ablation (SAP) is non-inferior to thermal endovenous ablation with concomitant phlebectomy (TAP), and whether SAP is a cost-effective alternative to TAP.
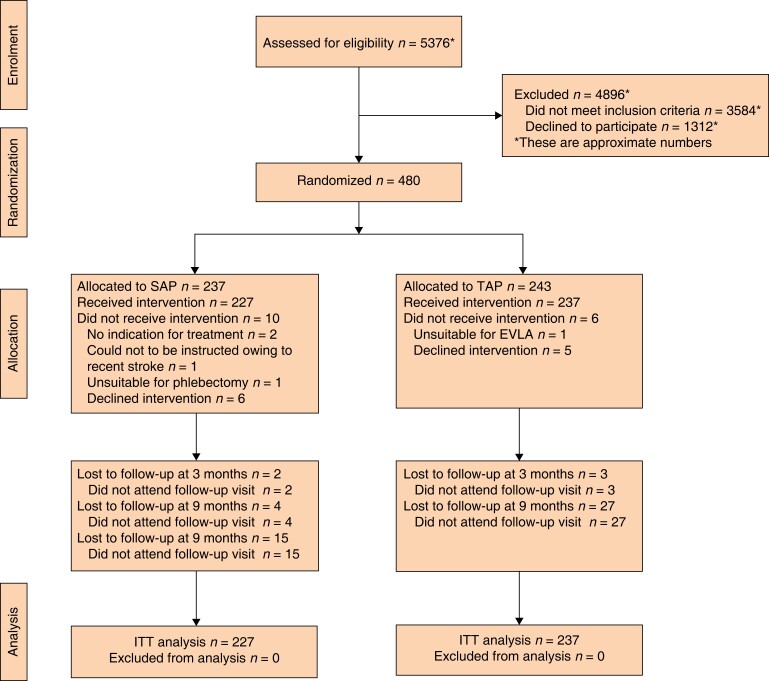
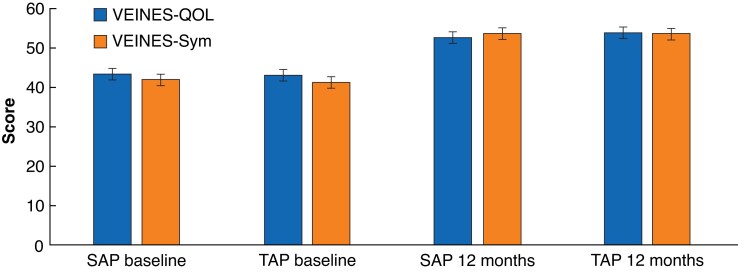
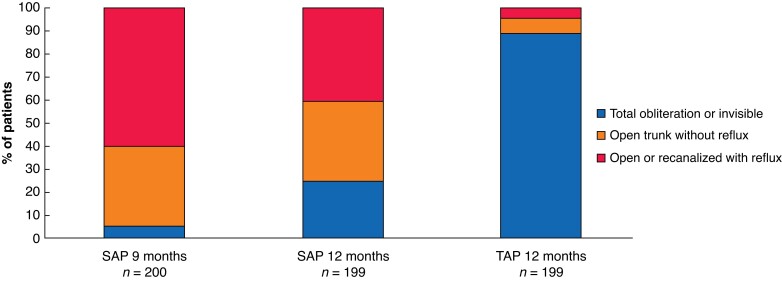
Methods: A multicentre, non-inferiority RCT was conducted in patients with an incompetent great saphenous vein or anterior accessory saphenous vein with one or more incompetent tributaries. Participants were randomized to receive SAP or TAP. After 9 months, additional truncal treatment was considered for SAP patients with remaining symptoms. The primary outcome was VEnous INsufficiency Epidemiological and Economic Study Quality of Life/Symptoms (VEINES-QOL/Sym score) after 12 months. Secondary outcomes were, among others, cost-effectiveness, perceived improvement of symptoms, and anatomical success.
Results: Some 464 patients received the allocated treatment (SAP 227, TAP 237). VEINES-QOL scores were 52.7 (95 per cent c.i. 51.9 to 53.9) for SAP and 53.8 (53.3 to 55.1) for TAP; VEINES-Sym scores were 53.5 (52.6 to 54.4) and 54.2 (54.0 to 55.6) respectively. Fifty-eight patients (25.6 per cent) in the SAP group received additional truncal ablation. Treatment with SAP was less costly than treatment with TAP.
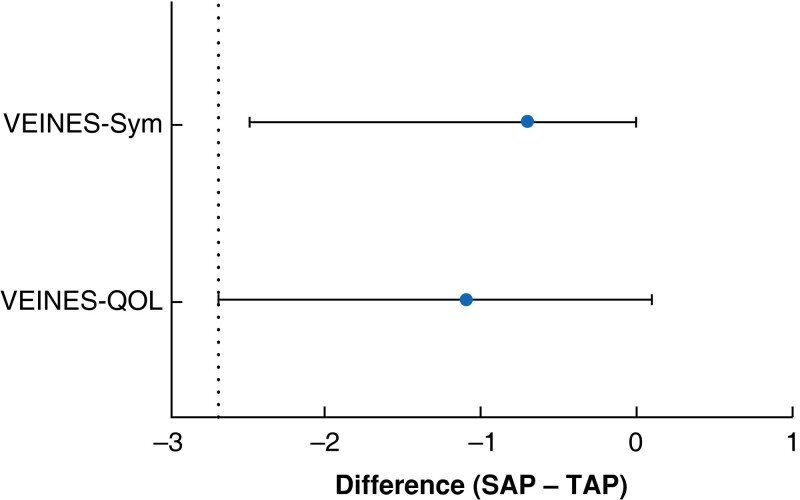
Conclusion: One year after treatment, participants who underwent SAP had non-inferior health-related quality of life compared with those who had TAP. Treatment with SAP was a cost-effective alternative to TAP at 12 months.
Registration number: NTR 4821 (www.trialregister.nl).
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures

Comment in
-
Comment on: A randomized clinical trial of isolated ambulatory phlebectomy versus saphenous thermal ablation with concomitant phlebectomy (SAPTAP trial).Br J Surg. 2023 Apr 12;110(5):616. doi: 10.1093/bjs/znad038. Br J Surg. 2023. PMID: 36806549 Free PMC article. No abstract available.
References
-
- Rabe E, Berboth G, Pannier F. Epidemiologie der chronischen venenkrankheiten. Wien Med Wochenschr 2016;166:260–263 - PubMed
-
- Rabe E, Guex JJ, Puskas A, Scuderi A, Fernandez Quesada F; VCP Coordinators . Epidemiology of chronic venous disorders in geographically diverse populations: results from the Vein Consult Program. Int Angiol 2012;31:105–115 - PubMed
-
- Aherne TM, Ryan EJ, Boland MR, McKevitt K, Hassanin A, Tubassam Met al. . Concomitant vs. staged treatment of varicose tributaries as an adjunct to endovenous ablation: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg 2020;60:430–442 - PubMed
-
- De Maeseneer MG, Kakkos SK, Aherne T, Baekgaard N, Black S, Blomgren L, et al. Editor's Choice - European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs. Eur J Vasc Endovasc Surg 2022;63:184-267. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
