

A scoping study of pulmonary paracoccidioidomycosis: severity classification based on radiographic and tomographic evaluation
- PMID: 36465893
- PMCID: PMC9704082
- DOI: 10.1590/1678-9199-JVATITD-2022-0053
A scoping study of pulmonary paracoccidioidomycosis: severity classification based on radiographic and tomographic evaluation
Abstract
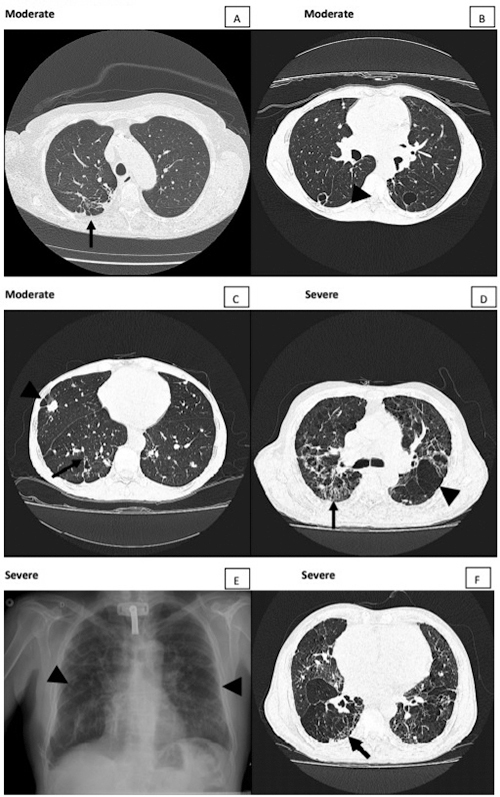
The lungs have great importance in patients with paracoccidioidomycosis since they are the portal of entry for the infecting fungi, the site of quiescent foci, and one of the most frequently affected organs. Although they have been the subject of many studies with different approaches, the severity classification of the pulmonary involvement, using imaging procedures, has not been carried out yet. This study aimed to classify the active and the residual pulmonary damage using radiographic and tomographic evaluations, according to the area involved and types of lesions.
Keywords: Paracoccidioides sp; Paracoccidioidomycosis; Radiographic evaluation; Severity classification.
Conflict of interest statement
Competing interests: The authors declare that they have no competing interests.
Figures
References
-
- Mendes RP. Paracoccidioidomycosis surveillance and control. J Venom Anim Toxins incl Trop Dis. 2010;16(2):194–197. doi: 10.1590/S1678-91992010000200003. - DOI
-
- Londero AT, Ramos CD. Paracoccidioidomycosis: a clinical and mycologic study of forty-one cases observed in Santa Maria, RS, Brazil. Am J Med. 1972;52(6):771–775. - PubMed
Publication types
LinkOut - more resources
Full Text Sources