

Distinct common signatures of gut microbiota associated with damp-heat syndrome in patients with different chronic liver diseases
- PMID: 36467028
- PMCID: PMC9712756
- DOI: 10.3389/fphar.2022.1027628
Distinct common signatures of gut microbiota associated with damp-heat syndrome in patients with different chronic liver diseases
Abstract
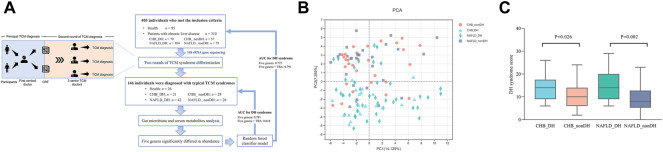
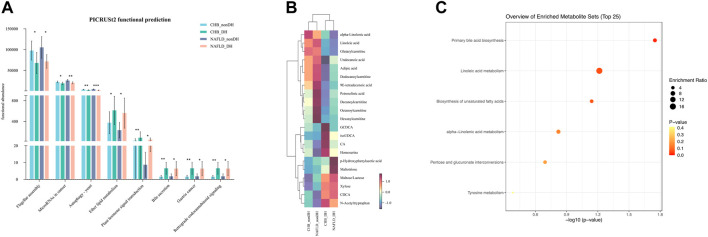
Background: Chronic hepatitis B (CHB) and non-alcoholic fatty liver disease (NAFLD) are prevalent in China. According to traditional Chinese medicine (TCM) theory, damp-heat (DH) syndrome is common in chronic liver disease. However, the biological characteristics related to quantitative diagnosis remain to be determined. This study aimed to identify the consistent alterations in the gut microbiota associated with DH syndrome in patients with CHB or NAFLD. Methods: A total of 405 individuals were recruited, of which 146 were participants who met the consistent TCM diagnosis by three senior TCM physicians and were typical syndromes. All participants were required to provide fresh stool and serum samples. The gut microbiota was assessed by fecal 16S rRNA gene sequencing, and the serum metabolite profiles of participants were quantified by an ultra-performance liquid chromatography coupled to tandem mass spectrometry (UPLC-MS/MS) system. DH syndrome-related bacteria taxa were identified based on the 146 individuals with typical syndromes and validated in all 405 volunteers. Results: The results showed that CHB and NAFLD patients with typical TCM DH syndrome had consistently elevated serum total bile acid (TBA) levels. Significant alterations in microbial community were observed according to TCM syndromes identification. A total of 870 microbial operational taxonomic units and 21 serum metabolites showed the same variation trends in both the CHB and NAFLD DH syndrome groups. The functional analysis predicts consistent dysregulation of bile acid metabolism. Five genera (Agathobacter, Dorea, Lachnospiraceae_NC2004_group, Subdoligranulum, and unclassified_c__Clostridia) significantly decreased in abundance in patients with DH syndrome. We utilize these five genera combined with TBA to construct a random forest classifier model to predict TCM diagnosis. The diagnostic receiver-operator characteristic (ROC) areas for DH syndrome were 0.818 and 0.791 in internal tenfold cross-validation and the test set based on all 405 individuals, respectively. Conclusion: There are common signatures of gut microbiota associated with DH syndrome in patients with different chronic liver diseases. Serum TBA combined with DH-related genera provides a good diagnostic potential for DH syndrome in chronic liver disease.
Keywords: chronic hepatitis B; damp-heat syndrome; gut microbiota; non-alcoholic fatty liver disease; traditional Chinese medicine.
Copyright © 2022 Pan, Guo, Hu, Xun, Zhang, Feng, Chen, Li, Liu, Hu and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources
Miscellaneous