

Gut-kidney axis in IgA nephropathy: Role on mesangial cell metabolism and inflammation
- PMID: 36467425
- PMCID: PMC9715425
- DOI: 10.3389/fcell.2022.993716
Gut-kidney axis in IgA nephropathy: Role on mesangial cell metabolism and inflammation
Abstract
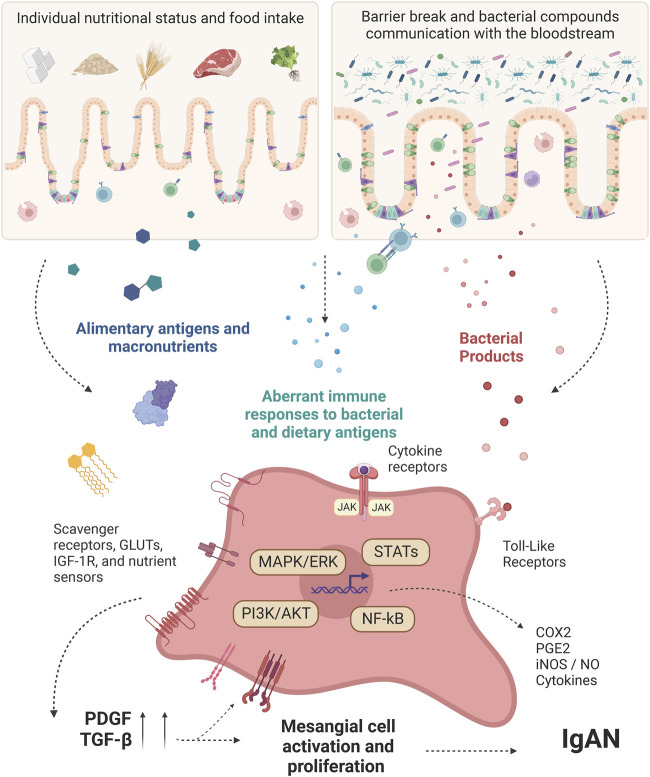
IgA Nephropathy (IgAN) is the commonest primary glomerular disease around the world and represents a significant cause of end-stage renal disease. IgAN is characterized by mesangial deposition of IgA-immune complexes and mesangial expansion. The pathophysiological process includes an abnormally glycosylated IgA1, which is an antigenic target. Autoantibodies specifically recognize galactose-deficient IgA1 forming immune complexes that are amplified in size by the soluble IgA Fc receptor CD89 leading to deposition in the mesangium through interaction with non-classical IgA receptors. The local production of cytokines promotes local inflammation and complement system activation, besides the stimulation of mesangial proliferation. The spectrum of clinical manifestations is quite variable from asymptomatic microscopic hematuria to rapidly progressive glomerulonephritis. Despite all the advances, the pathophysiology of the disease is still not fully elucidated. The mucosal immune system is quoted to be a factor in triggering IgAN and a "gut-kidney axis" is proposed in its development. Furthermore, many recent studies have demonstrated that food intake interferes directly with disease prognosis. In this review, we will discuss how mucosal immunity, microbiota, and nutritional status could be interfering directly with the activation of intrinsic pathways of the mesangial cells, directly resulting in changes in their function, inflammation and development of IgAN.
Keywords: IgA nephropathy; gut-kidney axis; kidney; mesangial cells; microbiota.
Copyright © 2022 Luvizotto, Menezes-Silva, Woronik, Monteiro and Câmara.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Soluble CD89 is a critical factor for mesangial proliferation in childhood IgA nephropathy.Kidney Int. 2022 Feb;101(2):274-287. doi: 10.1016/j.kint.2021.09.023. Epub 2021 Oct 28. Kidney Int. 2022. PMID: 34756952
-
Both IgA nephropathy and alcoholic cirrhosis feature abnormally glycosylated IgA1 and soluble CD89-IgA and IgG-IgA complexes: common mechanisms for distinct diseases.Kidney Int. 2011 Dec;80(12):1352-63. doi: 10.1038/ki.2011.276. Epub 2011 Aug 24. Kidney Int. 2011. PMID: 21866091
-
Murine Models of Human IgA Nephropathy.Semin Nephrol. 2018 Sep;38(5):513-520. doi: 10.1016/j.semnephrol.2018.05.021. Semin Nephrol. 2018. PMID: 30177023 Review.
-
IgA1 Protease Treatment Reverses Mesangial Deposits and Hematuria in a Model of IgA Nephropathy.J Am Soc Nephrol. 2016 Sep;27(9):2622-9. doi: 10.1681/ASN.2015080856. Epub 2016 Feb 5. J Am Soc Nephrol. 2016. PMID: 26850635 Free PMC article.
-
Role of IgA receptors in the pathogenesis of IgA nephropathy.J Nephrol. 2016 Feb;29(1):5-11. doi: 10.1007/s40620-015-0246-5. Epub 2015 Nov 14. J Nephrol. 2016. PMID: 26572664 Review.
Cited by
-
A PRoliferation-Inducing Ligand (APRIL) in the Pathogenesis of Immunoglobulin A Nephropathy: A Review of the Evidence.J Clin Med. 2023 Nov 4;12(21):6927. doi: 10.3390/jcm12216927. J Clin Med. 2023. PMID: 37959392 Free PMC article. Review.
-
Lactate programs PBX1 lactylation and mesangial proliferation in lupus nephritis.JCI Insight. 2025 Apr 29;10(11):e190838. doi: 10.1172/jci.insight.190838. eCollection 2025 Jun 9. JCI Insight. 2025. PMID: 40299657 Free PMC article.
-
Hirudin in the Treatment of Chronic Kidney Disease.Molecules. 2024 Feb 27;29(5):1029. doi: 10.3390/molecules29051029. Molecules. 2024. PMID: 38474541 Free PMC article. Review.
-
Characteristics, pathogenic and therapeutic role of gut microbiota in immunoglobulin A nephropathy.Front Immunol. 2025 Feb 6;16:1438683. doi: 10.3389/fimmu.2025.1438683. eCollection 2025. Front Immunol. 2025. PMID: 39981255 Free PMC article. Review.
-
Bibliometric analysis of mucosal immunity in IgA nephropathy from 1990 to 2022.Immun Inflamm Dis. 2024 Jan;12(1):e1156. doi: 10.1002/iid3.1156. Immun Inflamm Dis. 2024. PMID: 38270317 Free PMC article.
References
-
- Almroth G., Axelsson T., Müssener E., Grodzinsky E., Midhagen G., Olcén P. (2006). Increased prevalence of anti-gliadin IgA-antibodies with aberrant duodenal histopathological findings in patients with IgA-nephropathy and related disorders. Ups. J. Med. Sci. 111 (3), 339–352. 10.3109/2000-1967-060 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous