

Individualised prediction of drug resistance and seizure recurrence after medication withdrawal in people with juvenile myoclonic epilepsy: A systematic review and individual participant data meta-analysis
- PMID: 36467455
- PMCID: PMC9716332
- DOI: 10.1016/j.eclinm.2022.101732
Individualised prediction of drug resistance and seizure recurrence after medication withdrawal in people with juvenile myoclonic epilepsy: A systematic review and individual participant data meta-analysis
Abstract
Background: A third of people with juvenile myoclonic epilepsy (JME) are drug-resistant. Three-quarters have a seizure relapse when attempting to withdraw anti-seizure medication (ASM) after achieving seizure-freedom. It is currently impossible to predict who is likely to become drug-resistant and safely withdraw treatment. We aimed to identify predictors of drug resistance and seizure recurrence to allow for individualised prediction of treatment outcomes in people with JME.
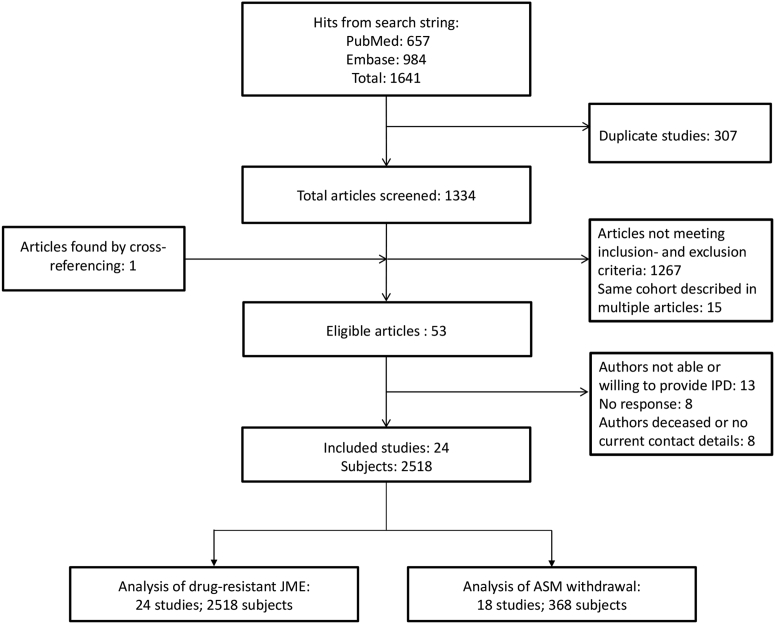
Methods: We performed an individual participant data (IPD) meta-analysis based on a systematic search in EMBASE and PubMed - last updated on March 11, 2021 - including prospective and retrospective observational studies reporting on treatment outcomes of people diagnosed with JME and available seizure outcome data after a minimum one-year follow-up. We invited authors to share standardised IPD to identify predictors of drug resistance using multivariable logistic regression. We excluded pseudo-resistant individuals. A subset who attempted to withdraw ASM was included in a multivariable proportional hazards analysis on seizure recurrence after ASM withdrawal. The study was registered at the Open Science Framework (OSF; https://osf.io/b9zjc/).
Findings: Our search yielded 1641 articles; 53 were eligible, of which the authors of 24 studies agreed to collaborate by sharing IPD. Using data from 2518 people with JME, we found nine independent predictors of drug resistance: three seizure types, psychiatric comorbidities, catamenial epilepsy, epileptiform focality, ethnicity, history of CAE, family history of epilepsy, status epilepticus, and febrile seizures. Internal-external cross-validation of our multivariable model showed an area under the receiver operating characteristic curve of 0·70 (95%CI 0·68-0·72). Recurrence of seizures after ASM withdrawal (n = 368) was predicted by an earlier age at the start of withdrawal, shorter seizure-free interval and more currently used ASMs, resulting in an average internal-external cross-validation concordance-statistic of 0·70 (95%CI 0·68-0·73).
Interpretation: We were able to predict and validate clinically relevant personalised treatment outcomes for people with JME. Individualised predictions are accessible as nomograms and web-based tools.
Funding: MING fonds.
Keywords: Drug resistance; Individual participant data; JME; Juvenile myoclonic epilepsy; Medication withdrawal; Meta-analysis; Multivariable prediction; Prediction model; Refractory epilepsy; Remission; Seizure recurrence.
© 2022 The Author(s).
Conflict of interest statement
AAA received a grant from the 10.13039/501100012155National Institute for Medical Research Development, royalties for a book publication from 10.13039/501100007723Oxford University Press, and speaker fees from Cobel Daruo, Tekaje, and Raymand Rad. CPB received research grants and honoraria from 10.13039/100011110UCB and 10.13039/501100003769Eisai, support for attending meetings by UCB, and served in the advisory board of Arvelle. CDB received consulting fees and honoraria from 10.13039/100014114GW Pharmaceuticals, 10.13039/100015661UCB Pharma, 10.13039/501100003769Eisai, 10.13039/501100006546Angelini Pharma and Bial. JPS received grants from the 10.13039/100000002National Institutes of Health, 10.13039/100000005Department of Defense, and the 10.13039/100000001National Science Foundation; and consulting fees from 10.13039/100015661UCB Pharma, AdCel Biopharma, LLC, iFovea, SK Life Sciences, and 10.13039/100013410LivaNova; and has stock options for iFovea and AdCel Biopharma. LEH-V participates in the Young Epilepsy Society, received speaker honorario from Armstrong, and was supported by Abbott pharmaceuticals to attend the Mexican Congress of Neurology. NP received honoraria from Zogenix and Ethos for Angelini Pharma. NS received honoraria from Biomarin, Livanova, GW Pharma, Zogenix and Marinus; and support to attend meetings from Livanova, GW Pharma and Zogenix; and participated on a data safety monitoring board for Marinus. SB received speaker fees from Eisai. PK received lecture honorarium from UCB Pharma and Eisai, consulting fees from 10.13039/501100003769Eisai and 10.13039/100013410LivaNova and his institution received research grants from 10.13039/100015661UCB Pharma and 10.13039/501100003769Eisai. MS received speaker honoraria from UCB Pharma and Eisai. KKS received research grants from the 10.13039/501100005416Norwegian Research Council, the DAMFoundation and the Norwegian National Advisory Unit on Rare diseases; and a networking grant from the 10.13039/501100004785NordForsk Foundation; and she acted as a paid PhD defense opponent at the University of Bergen, and attended a meeting for Nordic clinicians organised by Eisai. BJV received grants from the 10.13039/501100007870German Society for Epileptology and the 10.13039/501100001659Deutsche Forschungsgemeinschaft; and honoraria from University Medical Center Schleswig–Holstein and Cornelsen Verlag. MH received consulting fees and honoraria from Arvelle, Bial, Desitin, Eisai, GW Pharmaceuticals, UCB Pharma, and Zogenix. FvP has received speaker honoraria from Bial, Eisai, GW Pharmaceutical companies, Angelinipharma, Zogenix and UCB Pharma; and scientific advisory board honoraria from GW Pharmaceutical companies, UCB Pharma, and Angelinipharma. WD's salary is part-funded by The University of Melbourne; he has received travel, investigator-initiated, scientific advisory board and speaker honoraria from UCB Pharma Australia and Global; investigator-initiated, scientific advisory board, travel and speaker honoraria from Eisai Australia and Global; advisory board honoraria from Liva Nova and Tilray; educational grants from Novartis Pharmaceuticals, 10.13039/100014476Pfizer Pharmaceuticals and Sanofi-Synthelabo; educational; travel and fellowship grants from GSK Neurology Australia, and honoraria from SciGen Pharmaceuticals; and he has an equity interest in the device company EpiMinder. CPB received honaries and research support from EISAI, UCB and Arvelle. ET received speaker's honoraria from Arvelle, Abbott, Angelini Pharma, UCB, Biogen, Gerot-Lannacher, Bial, Eisai, Epilog, Takeda, Newbridge, Hikma, GW Pharmaceuticals, Sunovion Pharmaceuticals Inc., LivaNova and Novartis; consultancy funds from 10.13039/501100006546Angelini Pharma, Argenix, Arvelle, Epilog, 10.13039/100011110UCB, 10.13039/100005614Biogen, Gerot-Lannach, Bial, 10.13039/501100003769Eisai, 10.13039/100007723Takeda, Newbridge, 10.13039/100014114GW Pharmaceuticals, 10.13039/100009655Sunovion Pharmaceuticals Inc., Marinus, and 10.13039/100004336Novartis; directorship funds from Neuroconsult GmbH. ET's Institution received grants from 10.13039/100005614Biogen, Red Bull, 10.13039/100004334Merck, 10.13039/100011110UCB, 10.13039/501100000780European Union, FWF Österreichischer Fond zur Wissenschaftsförderung, and 10.13039/501100007148Bundesministerium für Wissenschaft und Forschung. JWS reports personal fees from Arvelle, personal fees from 10.13039/100011110UCB, grants from UCB, grants from 10.13039/100003997NEF, grants from UCB, personal fees from 10.13039/100012739Zogenix, grants from GW Phama, outside the submitted work; and his current position is endowed by the Epilepsy Society, he is a member of the Editorial Board of the Lancet Neurology, and receives research support from the Marvin Weil Epilepsy Research Fund. All other authors declare no potential competing interests. None of the above mentioned declarations represent a conflict of interest directly related to the present publication.
Figures



References
-
- Camfield C.S., Striano P., Camfield P.R. Epidemiology of juvenile myoclonic epilepsy. Epilepsy Behav. 2013;28(Suppl 1):S15–S17. - PubMed
-
- Proposal for revised classification of epilepsies and epileptic syndromes. Commission on classification and terminology of the international League against epilepsy. Epilepsia. 1989;30:389–399. - PubMed
-
- Koutroumanidis M., Arzimanoglou A., Caraballo R., et al. The role of EEG in the diagnosis and classification of the epilepsy syndromes: a tool for clinical practice by the ILAE Neurophysiology Task Force (Part 1) Epileptic Disord. 2017;19:233–298. - PubMed
-
- Kasteleijn-Nolst Trenité D.G.A., Schmitz B., Janz D., et al. Consensus on diagnosis and management of JME: from founder's observations to current trends. Epilepsy Behav. 2013;28(Suppl 1):S87–S90. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
