

Effect of dexamethasone on newborn survival at different administration-to-birth intervals: A secondary analysis of the WHO ACTION (Antenatal CorticosTeroids for Improving Outcomes in Preterm Newborn)-I trial
- PMID: 36467459
- PMCID: PMC9716334
- DOI: 10.1016/j.eclinm.2022.101744
Effect of dexamethasone on newborn survival at different administration-to-birth intervals: A secondary analysis of the WHO ACTION (Antenatal CorticosTeroids for Improving Outcomes in Preterm Newborn)-I trial
Abstract
Background: The WHO ACTION-I trial demonstrated that dexamethasone significantly reduced neonatal mortality when administered to women at risk of early preterm birth in low-resource countries. We conducted a secondary analysis to determine how these benefits can be optimised, by evaluating the effect of dexamethasone compared to placebo on newborn mortality and severe respiratory distress outcomes at different administration-to-birth intervals, and identifying the interval with the greatest benefits.
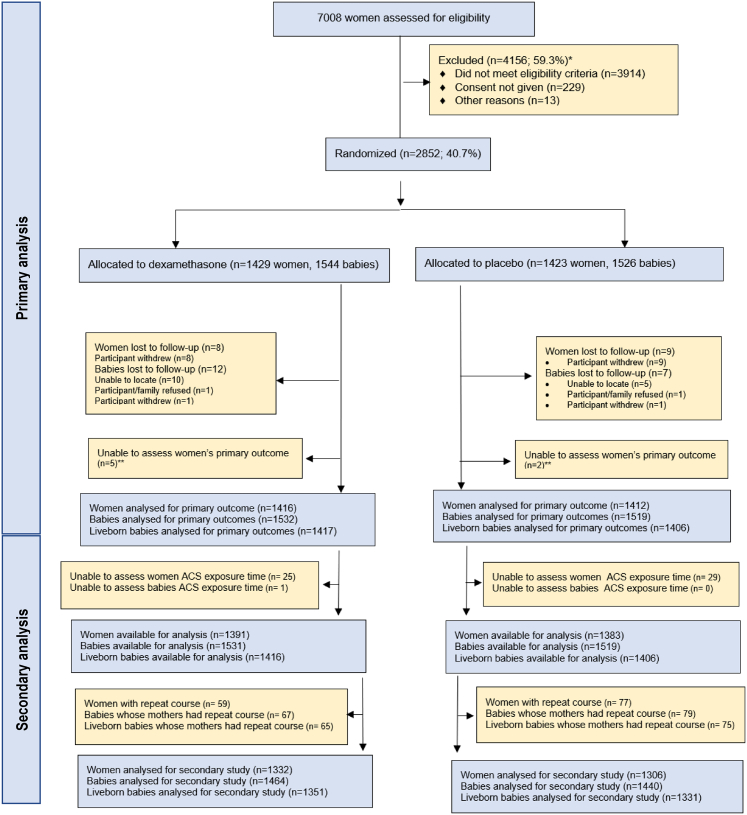
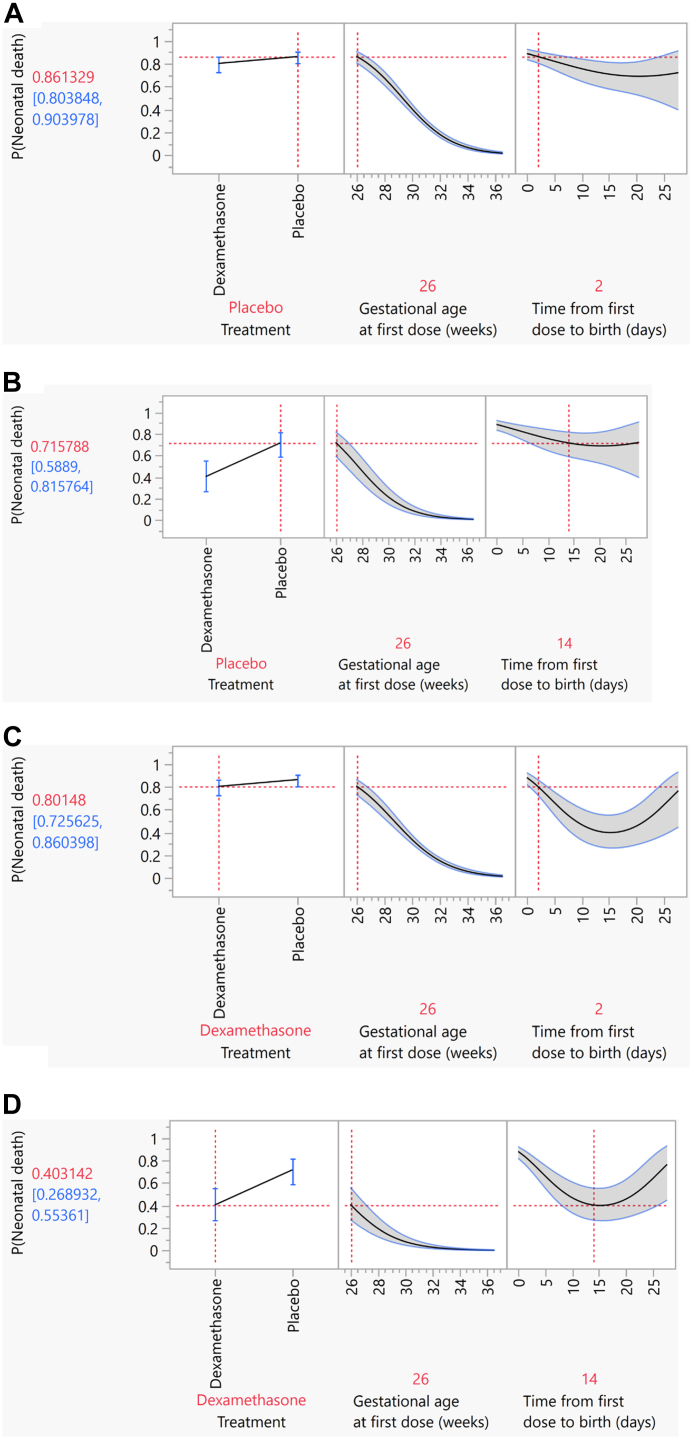
Methods: The WHO ACTION-I trial was a multi-country, individually-randomised, parallel-group, double-blind, placebo-controlled trial. It was conducted in 29 hospitals across Bangladesh, India, Kenya, Nigeria, and Pakistan. Women with a viable singleton or multiple pregnancy who presented to participating hospitals at a gestational age of 26 weeks 0 days-33 weeks 6 days and who were at risk of imminent preterm birth were eligible. In this secondary analysis, 2638 women and their newborns treated with single course of dexamethasone or placebo were analysed. Multivariate logistic regression was used to assess the effect of dexamethasone versus placebo on neonatal death, stillbirth or neonatal death, and severe respiratory distress at 24 h and at 168 h, by administration-to-birth interval (from 0 through 28 days), adjusting for gestational age at first dose. We used relative risks to identify the administration-to-birth interval with the greatest benefits of dexamethasone compared to placebo on the newborn outcomes.
Findings: Between 24 December 2017 and 21 November 2019, 2852 women and their 3070 babies were enrolled in the WHO ACTION-I trial; 1332 women (1464 babies) in the dexamethasone group and 1306 women (1440 babies) in the placebo group were included in this secondary analysis. Neonatal mortality risk was lower with increasing time between initiating dexamethasone and birth, achieving peak mortality reduction by days 13 and 14 and then diminishing as the interval approached 28 days, regardless of gestational age at administration. For other outcomes, the overall pattern of risk reduction extending into the second week was consistent with that of neonatal death.
Interpretation: In women at risk of preterm birth prior to 34 weeks' gestation, the neonatal benefits of antenatal dexamethasone appear to increase with longer administration-to-birth intervals than previously thought. This knowledge can support clinical assessment and estimation of the risks of adverse preterm newborn outcomes at the time of birth, and the potential benefits of antenatal dexamethasone treatment for a known administration-to-birth interval.
Funding: Bill and Melinda Gates Foundation; World Health Organization.
© 2022 World Health Organization.
Conflict of interest statement
All authors declare no competing interests.
Figures

Similar articles
-
The World Health Organization Antenatal CorTicosteroids for Improving Outcomes in preterm Newborns (ACTION-III) Trial: study protocol for a multi-country, multi-centre, double-blind, three-arm, placebo-controlled, individually randomized trial of antenatal corticosteroids for women at high probability of late preterm birth in hospitals in low- resource countries.Trials. 2024 Apr 12;25(1):258. doi: 10.1186/s13063-024-07941-0. Trials. 2024. PMID: 38609983 Free PMC article.
-
The World Health Organization ACTION-I (Antenatal CorTicosteroids for Improving Outcomes in preterm Newborns) Trial: a multi-country, multi-centre, two-arm, parallel, double-blind, placebo-controlled, individually randomized trial of antenatal corticosteroids for women at risk of imminent birth in the early preterm period in hospitals in low-resource countries.Trials. 2019 Aug 16;20(1):507. doi: 10.1186/s13063-019-3488-z. Trials. 2019. PMID: 31420064 Free PMC article. Clinical Trial.
-
Antenatal dexamethasone for late preterm birth: A multi-centre, two-arm, parallel, double-blind, placebo-controlled, randomized trial.EClinicalMedicine. 2022 Feb 12;44:101285. doi: 10.1016/j.eclinm.2022.101285. eCollection 2022 Feb. EClinicalMedicine. 2022. PMID: 35198915 Free PMC article.
-
Strategies for optimising antenatal corticosteroid administration for women with anticipated preterm birth.Cochrane Database Syst Rev. 2020 May 26;5(5):CD013633. doi: 10.1002/14651858.CD013633. Cochrane Database Syst Rev. 2020. PMID: 32452555 Free PMC article.
-
Antenatal corticosteroids beyond 34 weeks gestation: What do we do now?Am J Obstet Gynecol. 2016 Oct;215(4):423-30. doi: 10.1016/j.ajog.2016.06.023. Epub 2016 Jun 21. Am J Obstet Gynecol. 2016. PMID: 27342043 Review.
Cited by
-
Transdermal delivery of antenatal steroids to promote fetal lung maturation: Proof of principle data from sheep and non-human primate models.BMC Med. 2025 Aug 1;23(1):452. doi: 10.1186/s12916-025-04267-9. BMC Med. 2025. PMID: 40751152 Free PMC article.
-
Timing of Antenatal Corticosteroid Administration and Neonatal Outcomes.JAMA Netw Open. 2025 May 1;8(5):e2511315. doi: 10.1001/jamanetworkopen.2025.11315. JAMA Netw Open. 2025. PMID: 40388165 Free PMC article.
-
Impact of antenatal corticosteroids-to-delivery interval on very preterm neonatal outcomes: a retrospective study in two tertiary centers in Japan.BMC Pregnancy Childbirth. 2024 Sep 18;24(1):607. doi: 10.1186/s12884-024-06790-8. BMC Pregnancy Childbirth. 2024. PMID: 39294574 Free PMC article.
-
Effect of antenatal corticosteroid administration-to-birth interval on maternal and newborn outcomes: a systematic review.EClinicalMedicine. 2023 Mar 24;58:101916. doi: 10.1016/j.eclinm.2023.101916. eCollection 2023 Apr. EClinicalMedicine. 2023. PMID: 37007738 Free PMC article.
References
-
- World Health Organization . World Health Organization; Geneva: 2015. WHO recommendations on interventions to improve preterm birth outcomes. - PubMed
-
- Norman J., Shennan A., Jacobsson B., Stock S.J., FIGO Working Group for Preterm Birth FIGO good practice recommendations on the use of prenatal corticosteroids to improve outcomes and minimize harm in babies born preterm. Int J Gynaecol Obstet. 2021;155(1):26–30. - PubMed
LinkOut - more resources
Full Text Sources
