

A retrospective study on the characteristics of renal pathological grades in HSPN children with mild to moderate proteinuria
- PMID: 36467482
- PMCID: PMC9718029
- DOI: 10.3389/fped.2022.1029520
A retrospective study on the characteristics of renal pathological grades in HSPN children with mild to moderate proteinuria
Abstract
Objective: To investigate the characteristics of renal pathological grades in Henoch-Schönlein purpura nephritis (HSPN) children with mild to moderate proteinuria and the correlation between pathological grade and severity of proteinuria among this population.
Methods: HSPN children who were presented with mild (150 mg <24 h urinary protein <25 mg/kg) to moderate (25 mg/kg ≤24 h urinary protein <50 mg/kg) proteinuria and performed renal biopsy without steroid ± immunosuppressant treatment in the Second Xiangya Hospital between January 2010 and March 2021 were involved. We retrospectively analyzed the correlation between age, disease course, degree of proteinuria, type of immunoglobulin deposits, C3 deposits in glomeruli and renal pathological grade.
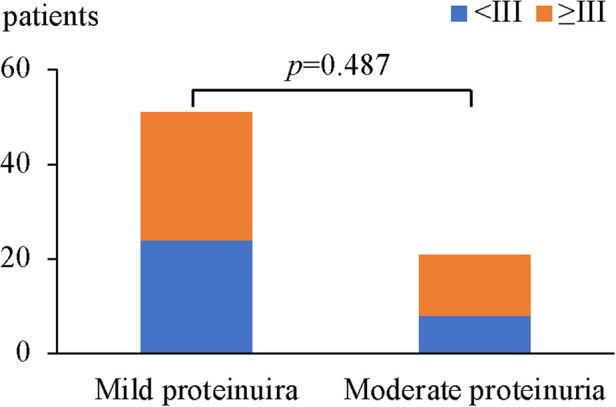
Results: (1) 72 HSPN children including 46 boys and 26 girls were included, with a mean age of onset of 9.01 ± 2.65 years old. The majority of these patients (62.5%) had a disease course between 1 week to 1 month. 51 patients presented with mild proteinuria and 21 patients with moderate proteinuria. (2) Renal biopsy results showed that ISKDC Grade IIIa were both predominant in mild proteinuria group (25, 49%) and moderate proteinuria group (11, 52.4%). 32 patients had grade II (44.4%), 2 had grade IIIb (2.8%), 1 had grade IV (1.4%), and 1 had grade VI (1.4%). There was no correlation between age, disease course and renal pathological grade (p > 0.05). (3) In patients with mild proteinuria (n = 51), 27 (52.9%) HSPN children had a pathological grade ≥ grade III. In patients with moderate proteinuria (n = 21), 13 (61.9%) HSPN children had grade ≥ III. There was no significant difference in the proportion of renal pathological grade between the 2 groups (p > 0.05). (4) There was no significant correlation between glomerular C3 deposits or immunoglobulin deposit types and renal pathological grade (p = 0.776 and p = 0.056 respectively).
Conclusion: In HSPN children with mild to moderate proteinuria, longer disease course or heavier urinary protein level is not completely parallel with higher renal pathological grade. ISKDC grade IIIa is the most common pathological grade. Clinicians should pay great attention to the renal injury in patients with mild to moderate proteinuria.
Keywords: Henoch–Schönlein purpura nephritis; children; immune complexes; proteinuria; renal pathology.
© 2022 Cao, Shen, Li, Shuai, Chen, Mo, Li, Li, Wang and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
[Relationship between clinical manifestations and renal pathology in children with Henoch-Schonlein purpura nephritis].Zhongguo Dang Dai Er Ke Za Zhi. 2007 Apr;9(2):129-32. Zhongguo Dang Dai Er Ke Za Zhi. 2007. PMID: 17448308 Chinese.
-
Correlation between endocapillary proliferative and nephrotic-range proteinuria in children with Henoch-Schönlein purpura nephritis.Pediatr Nephrol. 2019 Apr;34(4):663-670. doi: 10.1007/s00467-018-4134-9. Epub 2018 Nov 10. Pediatr Nephrol. 2019. PMID: 30415419
-
Podocalyxin expression in renal tissues and correlation with the number of urinary podocytes in children with Henoch-Schonlein purpura nephritis.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012 Feb;37(2):161-7. doi: 10.3969/j.issn.1672-7347.2012.02.009. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2012. PMID: 22561433
-
Henoch-Schönlein purpura nephritis in children: incidence, pathogenesis and management.World J Pediatr. 2015 Feb;11(1):29-34. doi: 10.1007/s12519-014-0534-5. Epub 2014 Dec 29. World J Pediatr. 2015. PMID: 25557596 Review.
-
Different histological classifications for Henoch-Schönlein purpura nephritis: which one should be used?Pediatr Rheumatol Online J. 2019 Feb 28;17(1):10. doi: 10.1186/s12969-019-0311-z. Pediatr Rheumatol Online J. 2019. PMID: 30819179 Free PMC article. Review.
Cited by
-
Clinicopathological features and prognosis of IgA vasculitis nephritis with nephrotic-range proteinuria in children.Pediatr Nephrol. 2024 Nov;39(11):3241-3250. doi: 10.1007/s00467-024-06441-2. Epub 2024 Jul 9. Pediatr Nephrol. 2024. PMID: 38980322
References
LinkOut - more resources
Full Text Sources
Miscellaneous