

Association of Hearing Aids and Cochlear Implants With Cognitive Decline and Dementia: A Systematic Review and Meta-analysis
- PMID: 36469314
- PMCID: PMC9856596
- DOI: 10.1001/jamaneurol.2022.4427
Association of Hearing Aids and Cochlear Implants With Cognitive Decline and Dementia: A Systematic Review and Meta-analysis
Abstract
Importance: Hearing loss is associated with cognitive decline. However, it is unclear if hearing restorative devices may have a beneficial effect on cognition.
Objective: To evaluate the associations of hearing aids and cochlear implants with cognitive decline and dementia.
Data sources: PubMed, Embase, and Cochrane databases for studies published from inception to July 23, 2021.
Study selection: Randomized clinical trials or observational studies published as full-length articles in peer-reviewed journals relating to the effect of hearing interventions on cognitive function, cognitive decline, cognitive impairment, and dementia in patients with hearing loss.
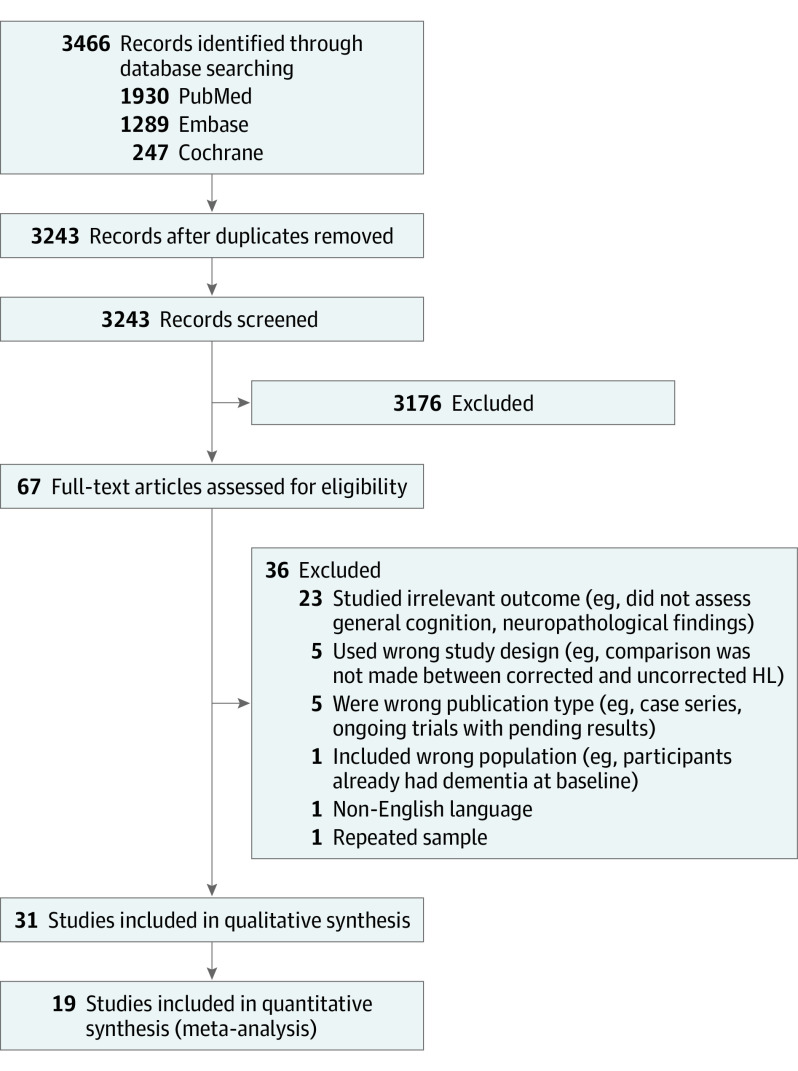
Data extraction and synthesis: The review was conducted in accordance with Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) reporting guidelines. Two authors independently searched the PubMed, Embase, and Cochrane databases for studies relating to the effect of hearing interventions on cognitive decline and dementia in patients with hearing loss.
Main outcomes and measures: Maximally adjusted hazard ratios (HRs) were used for dichotomous outcomes and ratio of means for continuous outcomes. Sources of heterogeneity were investigated using sensitivity and subgroup analyses, and publication bias was assessed using visual inspection, the Egger test, and trim and fill.
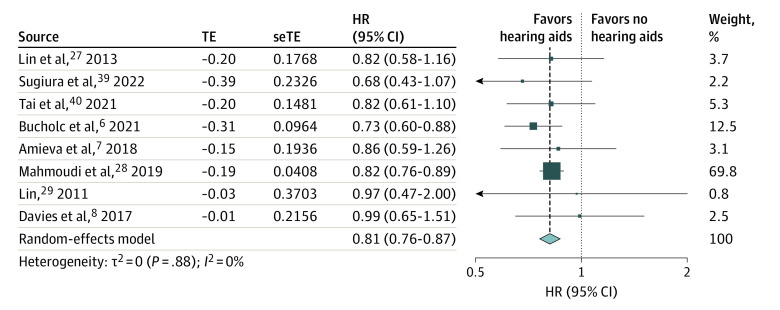
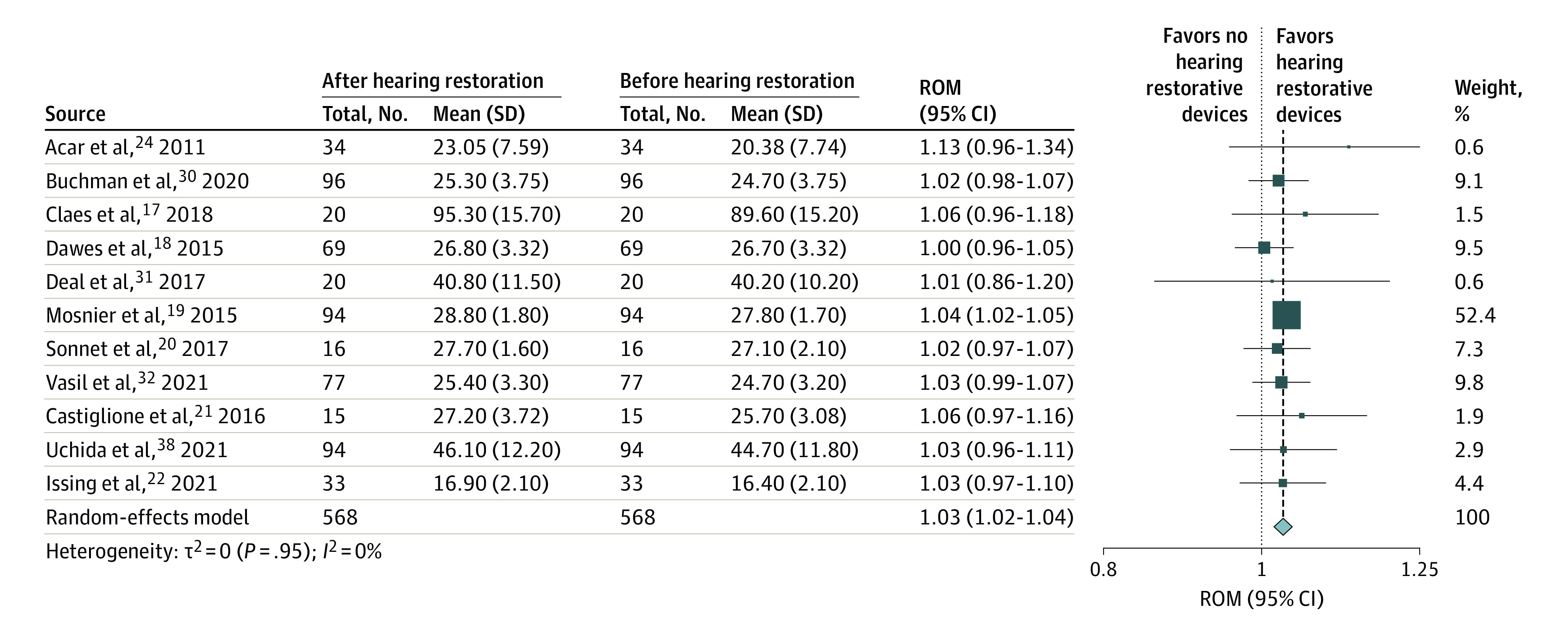
Results: A total of 3243 studies were screened; 31 studies (25 observational studies, 6 trials) with 137 484 participants were included, of which 19 (15 observational studies, 4 trials) were included in quantitative analyses. Meta-analysis of 8 studies, which had 126 903 participants, had a follow-up duration ranging from 2 to 25 years, and studied long-term associations between hearing aid use and cognitive decline, showed significantly lower hazards of any cognitive decline among hearing aid users compared with participants with uncorrected hearing loss (HR, 0.81; 95% CI, 0.76-0.87; I2 = 0%). Additionally, meta-analysis of 11 studies with 568 participants studying the association between hearing restoration and short-term cognitive test score changes revealed a 3% improvement in short-term cognitive test scores after the use of hearing aids (ratio of means, 1.03; 95% CI, 1.02-1.04, I2 = 0%).
Conclusions and relevance: In this meta-analysis, the usage of hearing restorative devices by participants with hearing loss was associated with a 19% decrease in hazards of long-term cognitive decline. Furthermore, usage of these devices was significantly associated with a 3% improvement in cognitive test scores that assessed general cognition in the short term. A cognitive benefit of hearing restorative devices should be further investigated in randomized trials.
Conflict of interest statement
Figures
Comment in
-
Hearing Aids and Cochlear Implants in the Prevention of Cognitive Decline and Dementia-Breaking Through the Silence.JAMA Neurol. 2023 Feb 1;80(2):127-128. doi: 10.1001/jamaneurol.2022.4155. JAMA Neurol. 2023. PMID: 36469311 No abstract available.
