

Provider beliefs in effectiveness and recommendations for primary HPV testing in 3 health-care systems
- PMID: 36469348
- PMCID: PMC9825247
- DOI: 10.1093/jncics/pkac086
Provider beliefs in effectiveness and recommendations for primary HPV testing in 3 health-care systems
Abstract
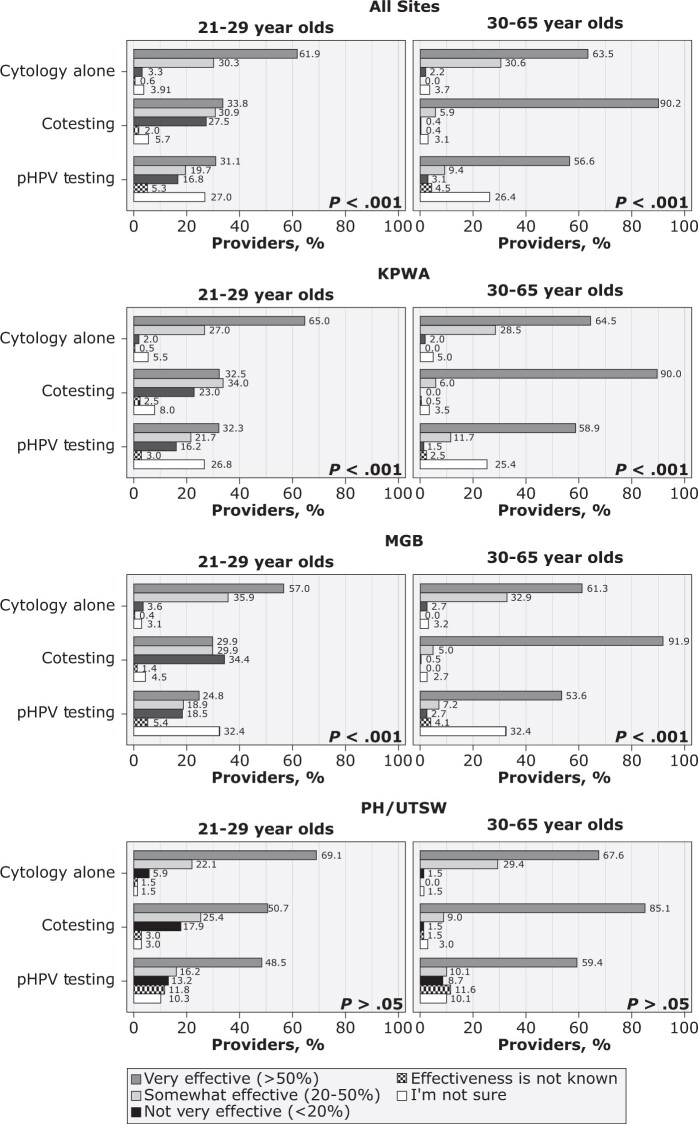
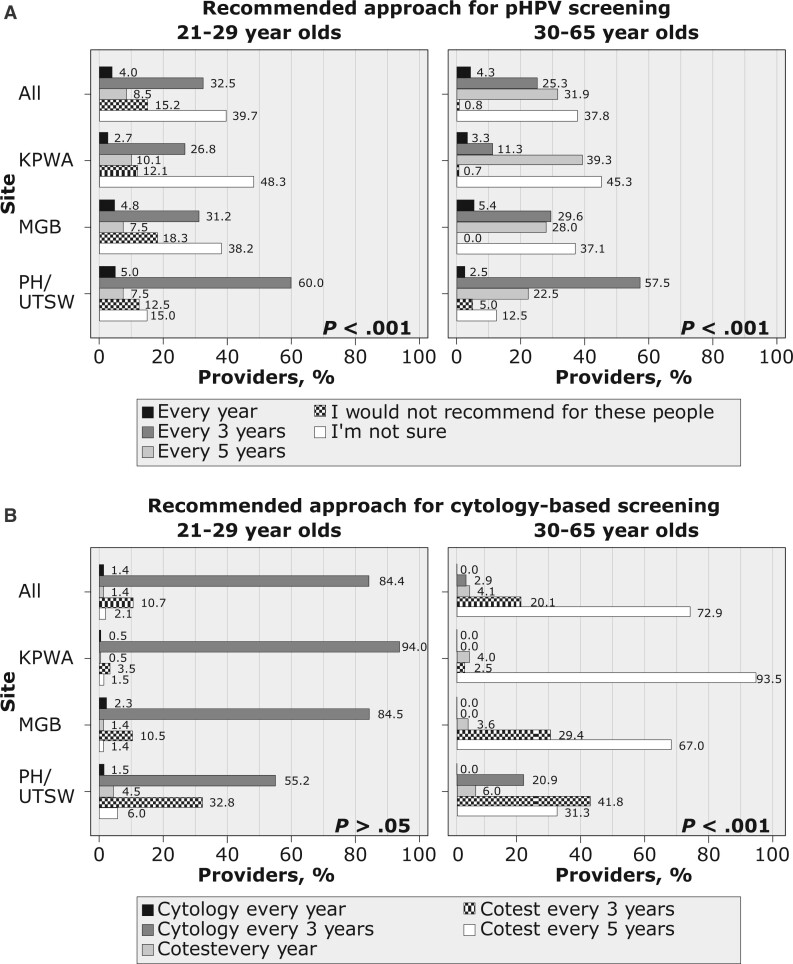
In 2018, the US Preventive Services Task Force endorsed primary human papillomavirus testing (pHPV) for cervical cancer screening. We aimed to describe providers' beliefs about pHPV testing effectiveness and which screening approach they regularly recommend. We invited providers who performed 10 or more cervical cancer screens in 2019 in 3 healthcare systems that had not adopted pHPV testing: Kaiser Permanente Washington, Mass General Brigham, and Parkland Health; 53.7% (501/933) completed the survey between October and December 2020. Response distributions varied across modalities (P < .001), with cytology alone or cotesting being more often viewed as somewhat or very effective for 30- to 65-year-olds compared with pHPV (cytology alone 94.1%, cotesting 96.1%, pHPV 66.0%). In 21- to 29-year-olds, the pattern was similar (cytology alone 92.2%, 64.7% cotesting, 50.8% pHPV). Most providers were either incorrect or unsure of the guideline-recommended screening interval for pHPV. Educational efforts are needed about the relative effectiveness and recommended use of pHPV to promote guideline-concordant care.
© The Author(s) 2022. Published by Oxford University Press.
Figures
References
-
- Haas JS, Sprague BL, Klabunde CN, et al. ; PROSPR (Population-based Research Optimizing Screening through Personalized Regimens) Consortium. Provider attitudes and screening practices following changes in breast and cervical cancer screening guidelines. J Gen Intern Med. 2016;31(1):52-59. - PMC - PubMed