

Circulating markers of inflammation and angiogenesis and clinical outcomes across subtypes of pulmonary arterial hypertension
- PMID: 36470771
- PMCID: PMC9840657
- DOI: 10.1016/j.healun.2022.10.026
Circulating markers of inflammation and angiogenesis and clinical outcomes across subtypes of pulmonary arterial hypertension
Abstract
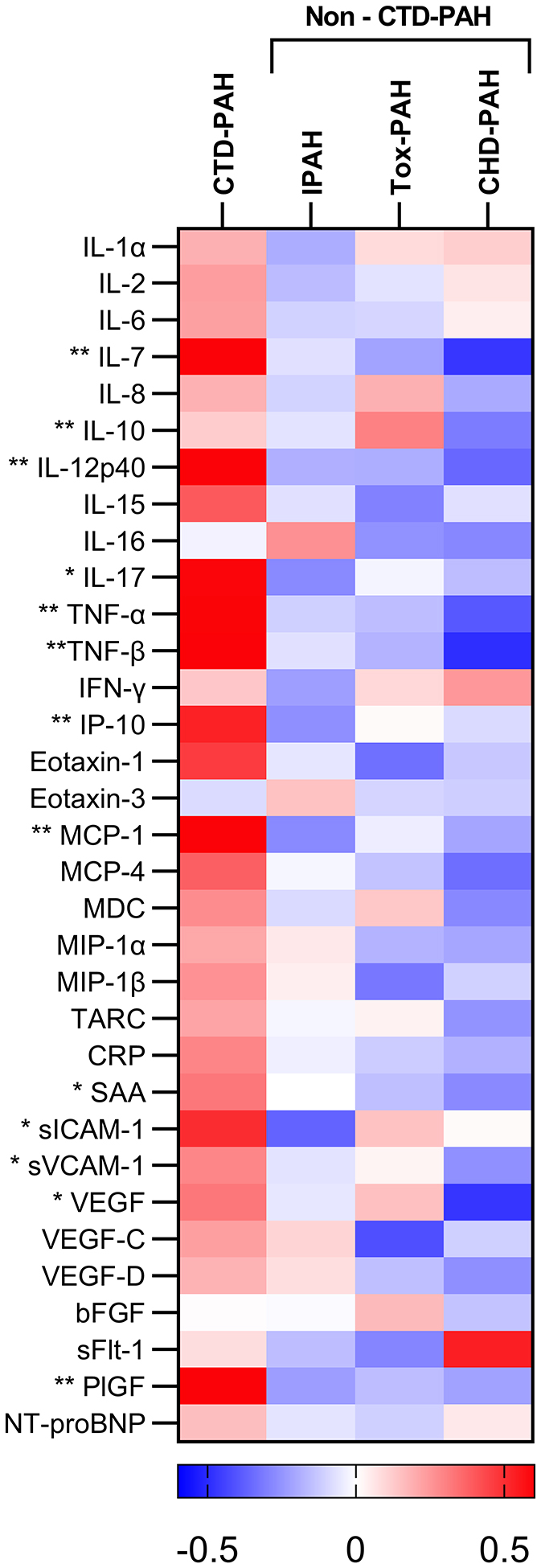
Background: Subtypes of pulmonary arterial hypertension (PAH) differ in both fundamental disease features and clinical outcomes. Angiogenesis and inflammation represent disease features that may differ across subtypes and are of special interest in connective tissue disease-associated PAH (CTD-PAH). We compared inflammatory and angiogenic biomarker profiles across different etiologies of PAH and related them to clinical outcomes.
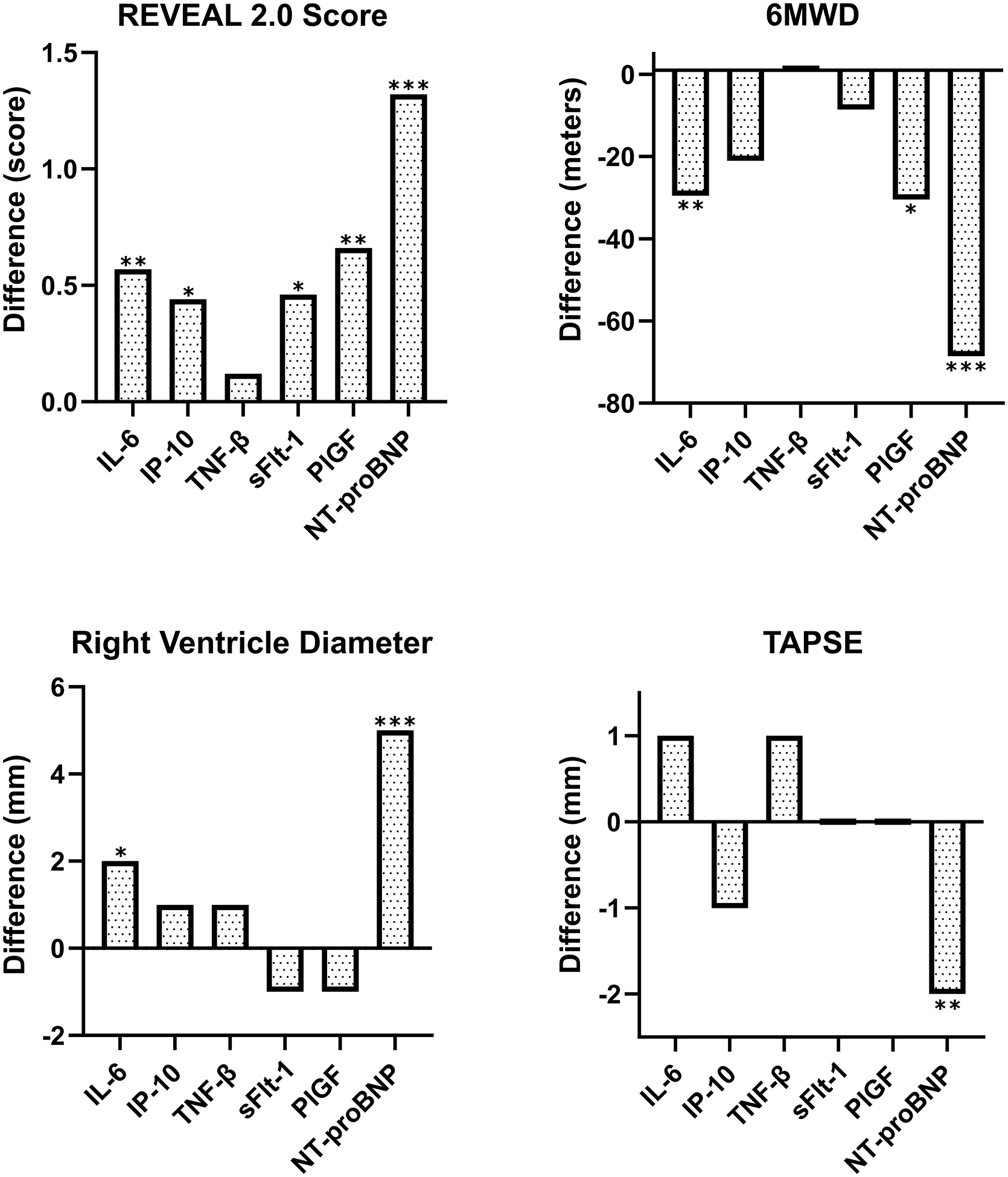
Methods: Participants with idiopathic PAH, CTD-PAH, toxin-associated PAH (tox-PAH), or congenital heart disease-associated PAH (CHD-PAH) were enrolled into a prospective observational cohort. Baseline serum concentrations of 33 biomarkers were related to 3-year mortality, echocardiogram, REVEAL score, and 6-minute walk distance (6MWD). Findings were validated using plasma proteomic data from the UK PAH Cohort Study.
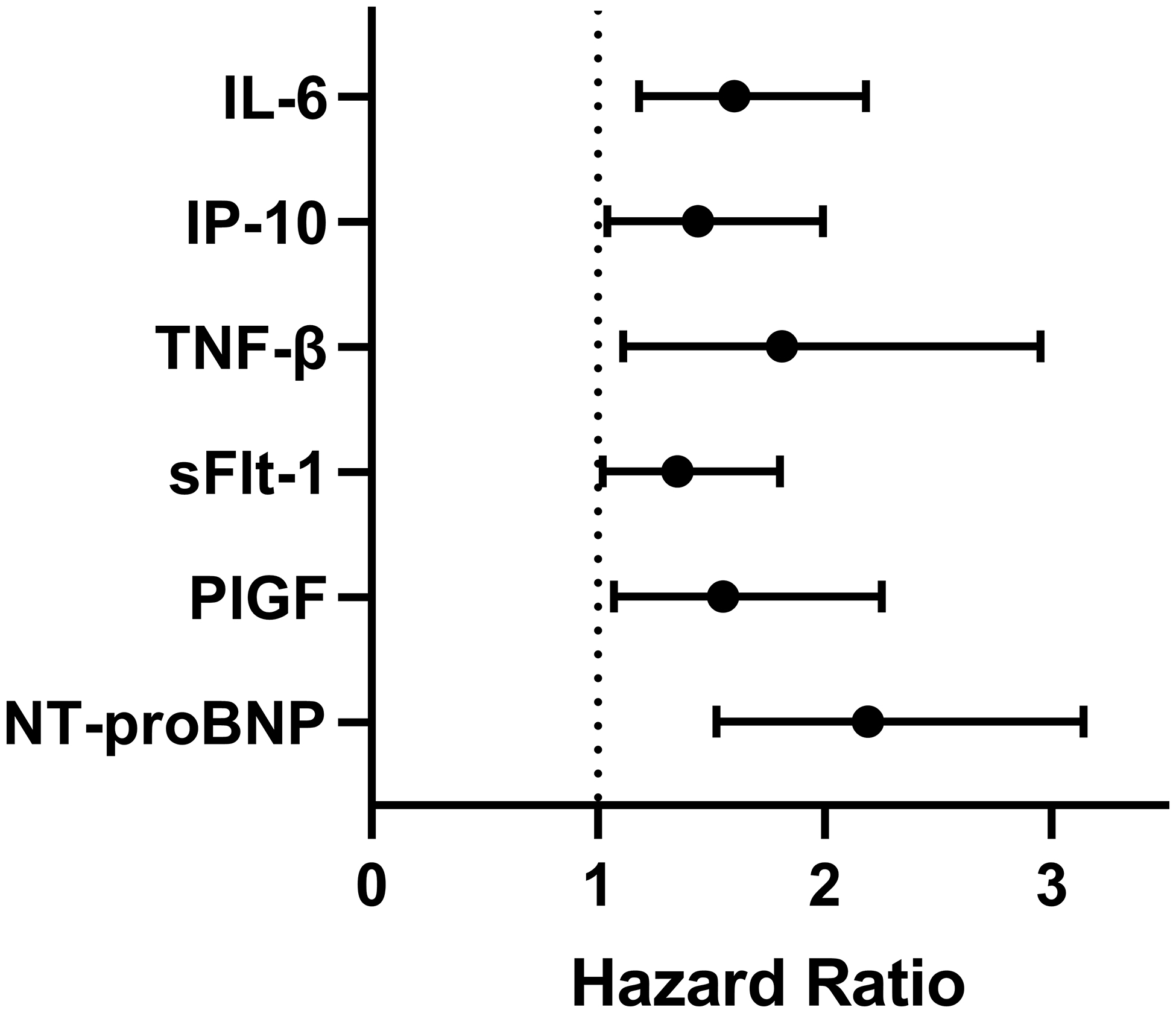
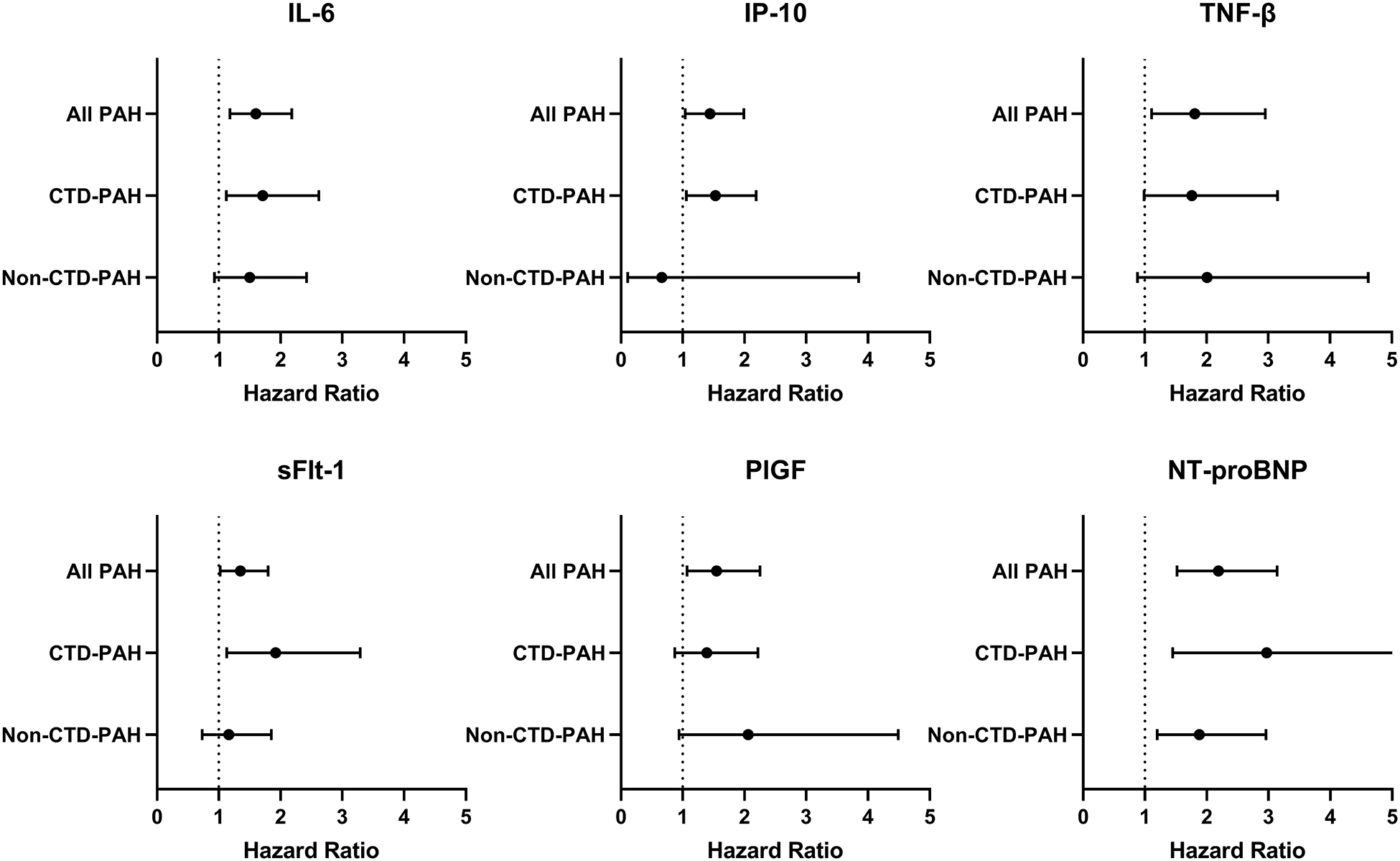
Results: One hundred twelve patients were enrolled: 45 idiopathic, 27 CTD-PAH, 20 tox-PAH, and 20 CHD-PAH. Angiogenic and inflammatory biomarkers were distinctly elevated within the CTD-PAH cohort. Six biomarkers were associated with mortality within the entire PAH cohort: interleukin-6 (IL-6, HR:1.6, 95% CI:1.18-2.18), soluble fms-like tyrosine kinase 1 (sFlt-1, HR:1.35, 95% CI:1.02-1.80), placental growth factor (PlGF, HR:1.55, 95% CI:1.07-2.25), interferon gamma-induced protein 10 (IP-10, HR:1.44, 95% CI:1.04-1.99), tumor necrosis factor-beta (TNF-β, HR:1.81, 95% CI:1.11-2.95), and NT-proBNP (HR:2.19, 95% CI:1.52-3.14). Only IL-6 and NT-proBNP remained significant after controlling for multiple comparisons. IL-6, IP-10, and sFlt-1 significantly associated with mortality in CTD-PAH, but not non-CTD-PAH subgroups. In the UK cohort, IP-10, PlGF, TNF-β, and NT-proBNP significantly associated with 5-year survival.
Conclusion: Levels of angiogenic and inflammatory biomarkers are elevated in CTD-PAH, compared with other etiologies of PAH, and may correlate with clinical outcomes including mortality.
Keywords: angiogenesis; biomarkers; connective tissue disease; etiology subtypes; inflammation; pulmonary arterial hypertension.
Copyright © 2022 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
