

Proteogenomic characterization of MiT family translocation renal cell carcinoma
- PMID: 36470859
- PMCID: PMC9722939
- DOI: 10.1038/s41467-022-34460-w
Proteogenomic characterization of MiT family translocation renal cell carcinoma
Abstract
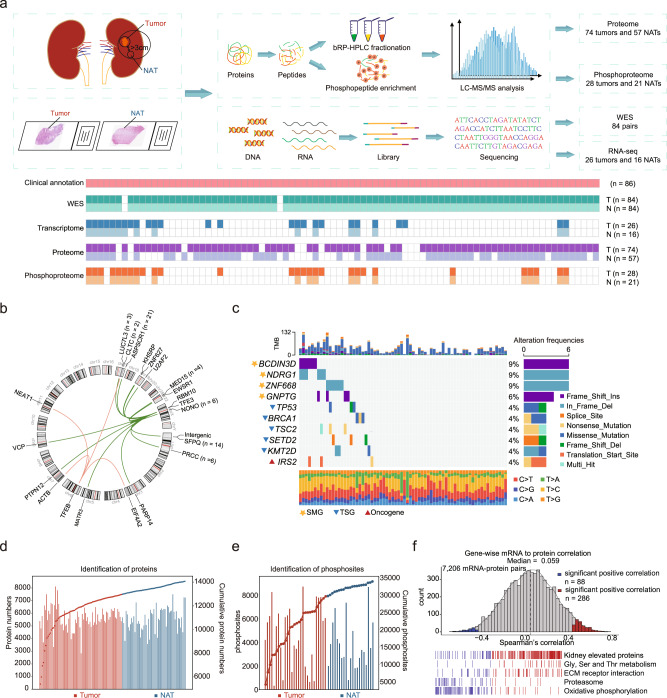
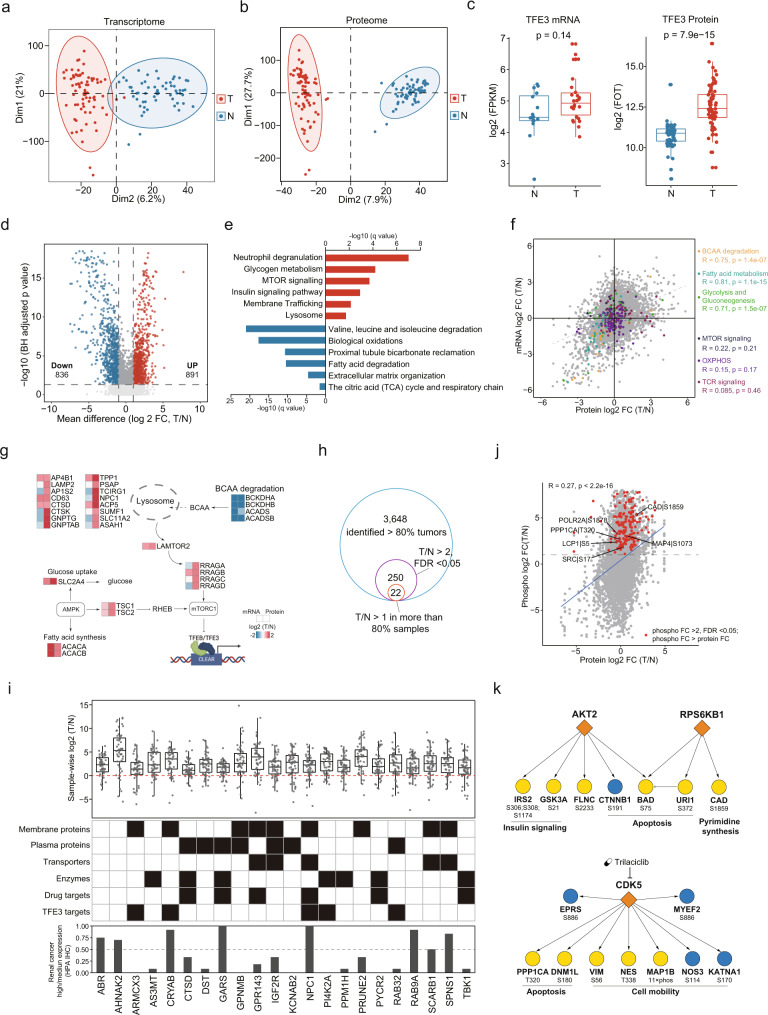
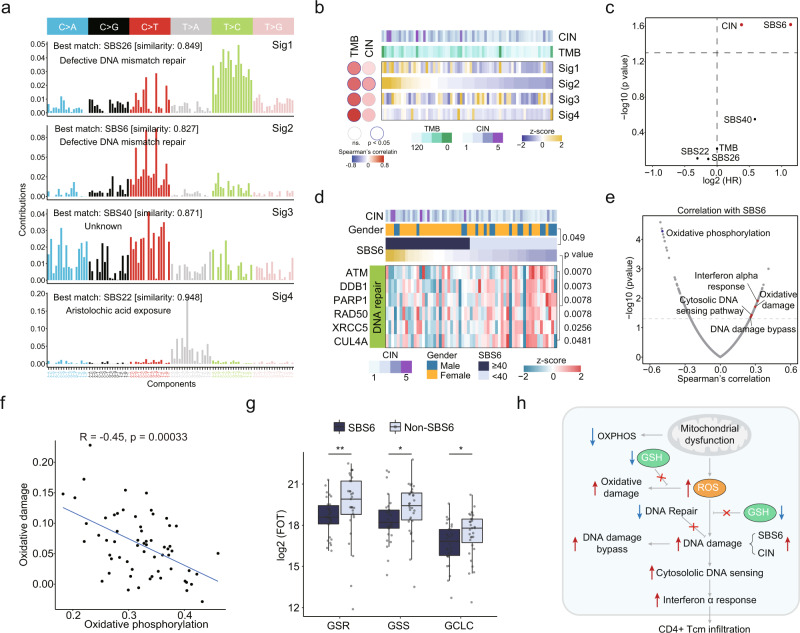
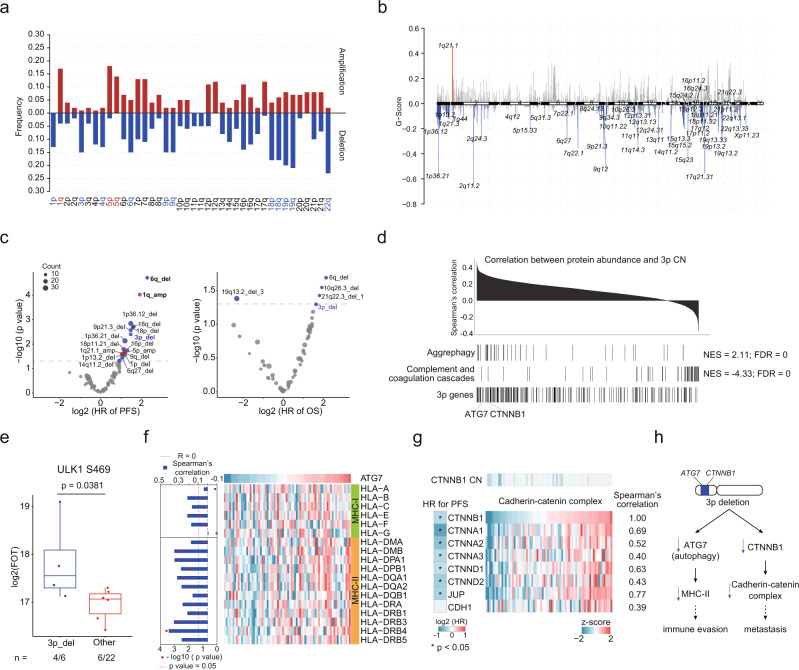
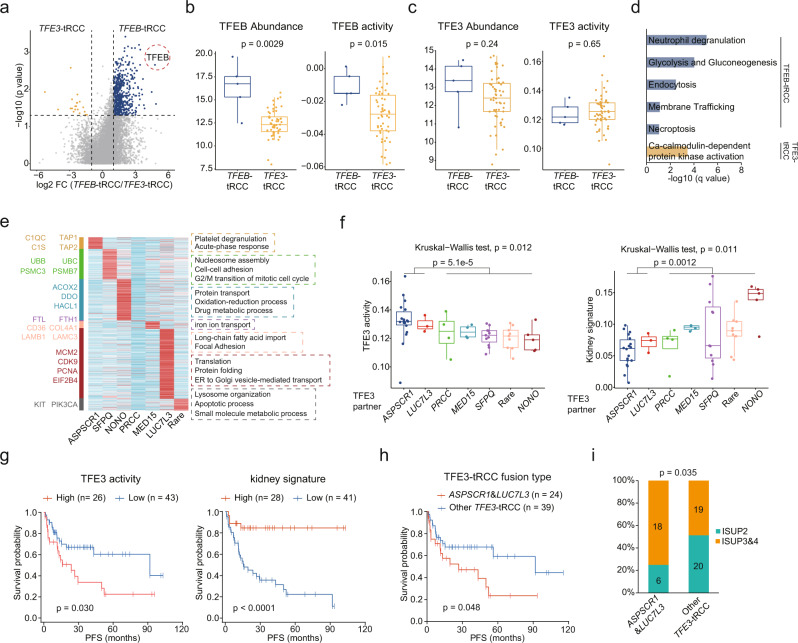
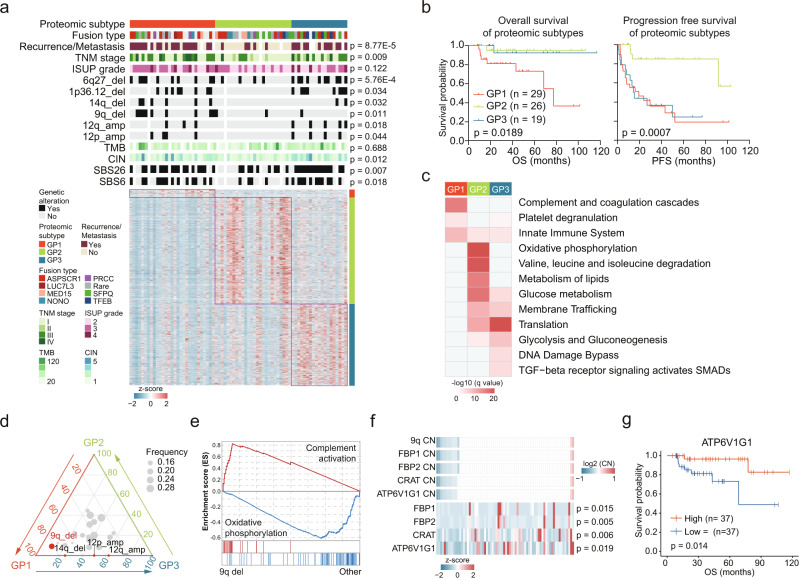
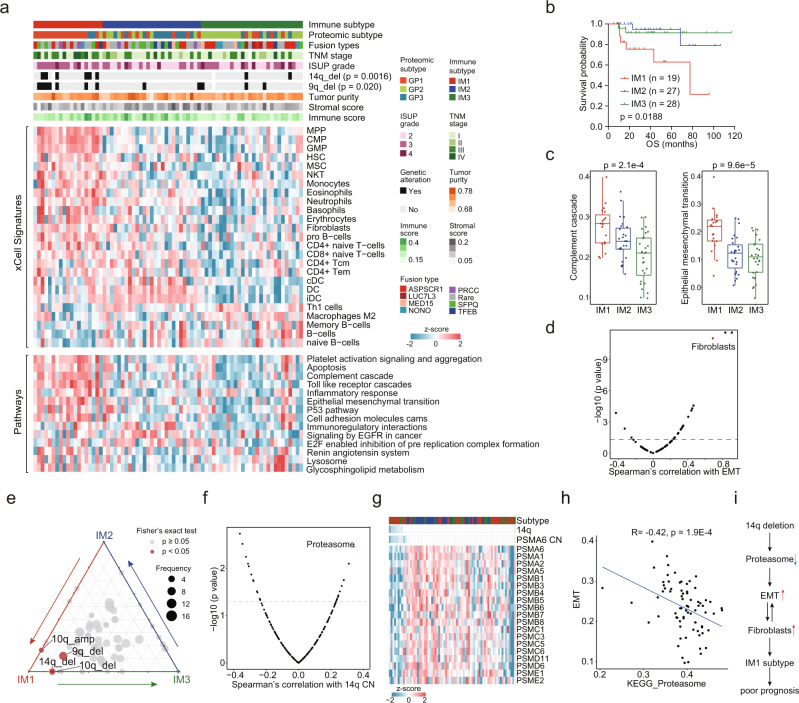
Microphthalmia transcription factor (MiT) family translocation renal cell carcinoma (tRCC) is a rare type of kidney cancer, which is not well characterized. Here we show the comprehensive proteogenomic analysis of tRCC tumors and normal adjacent tissues to elucidate the molecular landscape of this disease. Our study reveals that defective DNA repair plays an important role in tRCC carcinogenesis and progression. Metabolic processes are markedly dysregulated at both the mRNA and protein levels. Proteomic and phosphoproteome data identify mTOR signaling pathway as a potential therapeutic target. Moreover, molecular subtyping and immune infiltration analysis characterize the inter-tumoral heterogeneity of tRCC. Multi-omic integration reveals the dysregulation of cellular processes affected by genomic alterations, including oxidative phosphorylation, autophagy, transcription factor activity, and proteasome function. This study represents a comprehensive proteogenomic analysis of tRCC, providing valuable insights into its biological mechanisms, disease diagnosis, and prognostication.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Molecular characterization of tRCC.Nat Rev Urol. 2023 Feb;20(2):65. doi: 10.1038/s41585-022-00714-x. Nat Rev Urol. 2023. PMID: 36600088 No abstract available.
References
-
- Srigley, J. R. et al. The international society of urological pathology (ISUP) vancouver classification of renal neoplasia. 37, 1469–1489, (2013). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
