

Noncontiguous Multifocal Spondylodiscitis in 3 Regions of the Spine
- PMID: 36471773
- PMCID: PMC9719436
- DOI: 10.1155/2022/2091676
Noncontiguous Multifocal Spondylodiscitis in 3 Regions of the Spine
Abstract
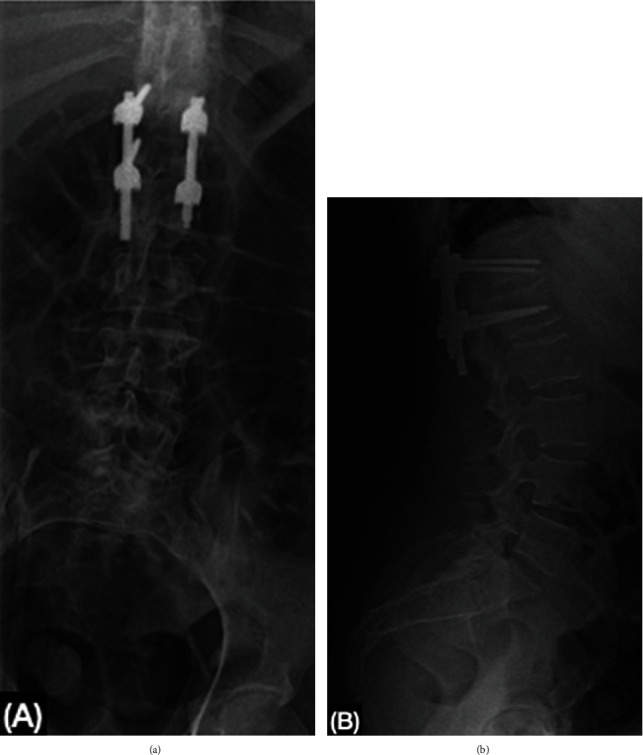
Spondylodiscitis is an uncommon infectious disease of the spine, usually presenting in 1 or 2 contiguous levels, associated with risk factors such as diabetes, intravenous drugs, corticosteroids, and invasive procedures. The most common presentation is pain with nonspecific systemic manifestations. Diagnosis relies on clinical suspicion, laboratories, and imaging studies. Urgent treatment is important due to the high morbid mortality associated with sepsis or a fulminant disease course. We report the case of a 39-year-old female diagnosed with noncontiguous multifocal spondylodiscitis, in the cervical, thoracic, and lumbar spine. The patient initially presented with back pain, inability to walk and severe neurological deficit in the upper and lower extremities, upon diagnosis broad-spectrum antibiotics were initiated. A staged surgical approach was performed in the 3 spine segments. During the 6 month follow-up, the patient presented walking with assistance, with the recovery of strength in the upper and lower extremities.
Copyright © 2022 Fernando González González et al.
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this manuscript.
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
