

Acute Pancreatitis Recurrences Augment Long-Term Pancreatic Cancer Risk
- PMID: 36473072
- PMCID: PMC10045975
- DOI: 10.14309/ajg.0000000000002081
Acute Pancreatitis Recurrences Augment Long-Term Pancreatic Cancer Risk
Abstract
Introduction: In animal models, inflammation caused by experimental acute pancreatitis (AP) promotes pancreatic carcinogenesis that is preventable by suppressing inflammation. Recent studies noted higher long-term risk of pancreatic ductal adenocarcinoma (PDAC) after AP. In this study, we evaluated whether the long-term PDAC risk after AP was influenced by the etiology of AP, number of recurrences, and if it was because of progression to chronic pancreatitis (CP).
Methods: This retrospective study used nationwide Veterans Administration database spanning 1999-2015. A 2-year washout period was applied to exclude patients with preexisting AP and PDAC. PDAC risk was estimated in patients with AP without (AP group) and with underlying CP (APCP group) and those with CP alone (CP group) and compared with PDAC risk in patients in a control group, respectively, using cause-specific hazards model.
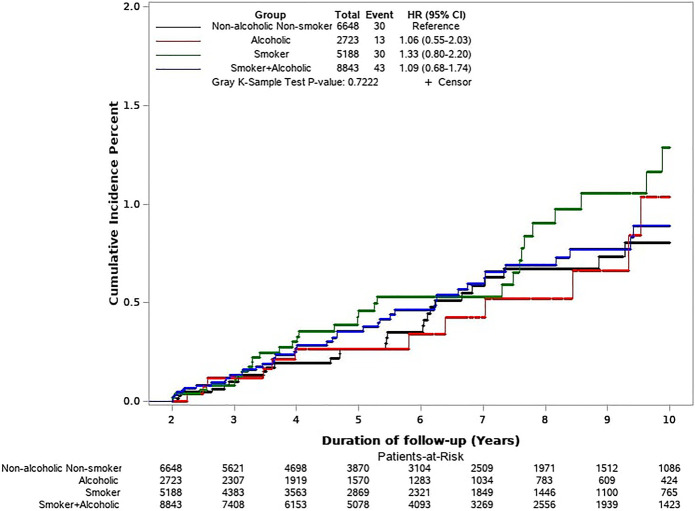
Results: The final cohort comprised 7,147,859 subjects (AP-35,550 and PDAC-16,475). The cumulative PDAC risk 3-10 years after AP was higher than in controls (0.61% vs 0.18%), adjusted hazard ratio (1.7 [1.4-2.0], P < 0.001). Adjusted hazard ratio was 1.5 in AP group, 2.4 in the CP group, and 3.3 in APCP group. PDAC risk increased with the number of AP episodes. Elevated PDAC risk after AP was not influenced by the etiology of AP (gallstones, smoking, or alcohol).
Discussion: There is a higher PDAC risk 3-10 years after AP irrespective of the etiology of AP, increases with the number of episodes of AP and is additive to higher PDAC risk because of CP.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures




References
-
- How Common Is Pancreatic Cancer? The American Cancer Society; (https://www.cancer.org/cancer/pancreatic-cancer/about/key-statistics.html) (2022). (Accessed January 7, 2022).
-
- Agarwal B, Correa AM, Ho L. Survival in pancreatic carcinoma based on tumor size. Pancreas 2008;36(1):e15–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
