

Nivolumab Plus Ipilimumab Versus EXTREME Regimen as First-Line Treatment for Recurrent/Metastatic Squamous Cell Carcinoma of the Head and Neck: The Final Results of CheckMate 651
- PMID: 36473143
- PMCID: PMC10115555
- DOI: 10.1200/JCO.22.00332
Nivolumab Plus Ipilimumab Versus EXTREME Regimen as First-Line Treatment for Recurrent/Metastatic Squamous Cell Carcinoma of the Head and Neck: The Final Results of CheckMate 651
Abstract
Purpose: CheckMate 651 (ClinicalTrials.gov identifier: NCT02741570) evaluated first-line nivolumab plus ipilimumab versus EXTREME (cetuximab plus cisplatin/carboplatin plus fluorouracil ≤ six cycles, then cetuximab maintenance) in recurrent/metastatic squamous cell carcinoma of the head and neck (R/M SCCHN).
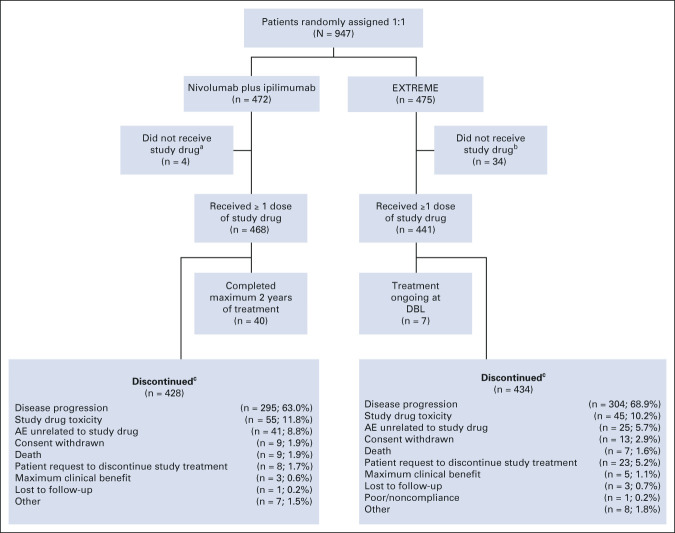
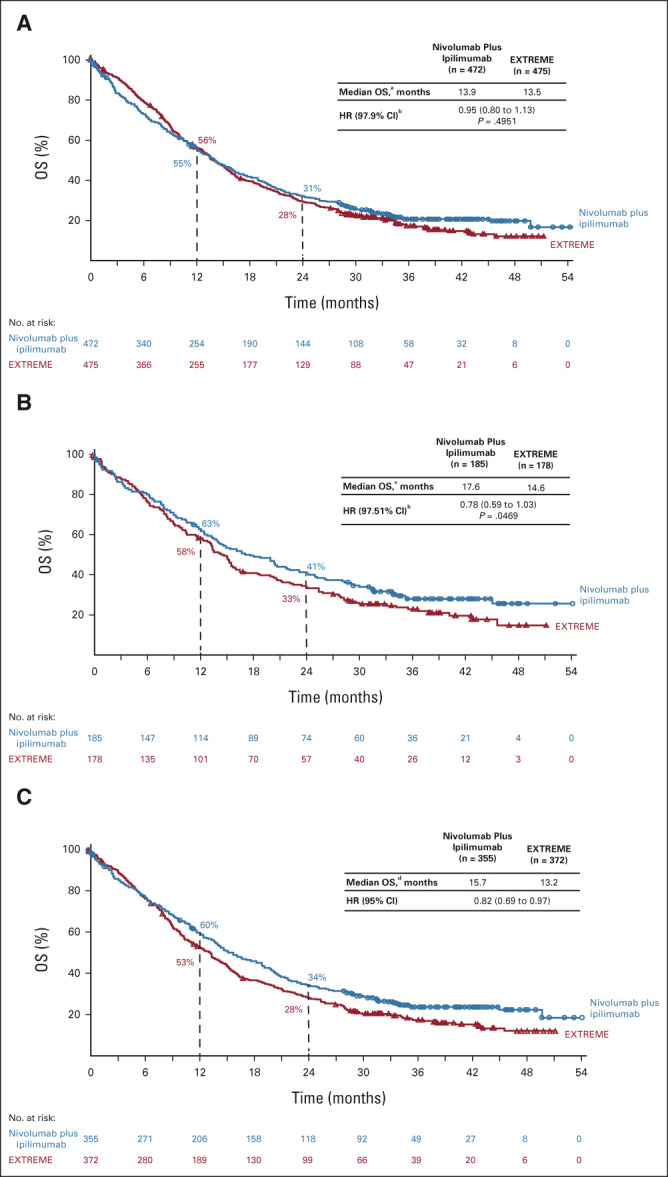
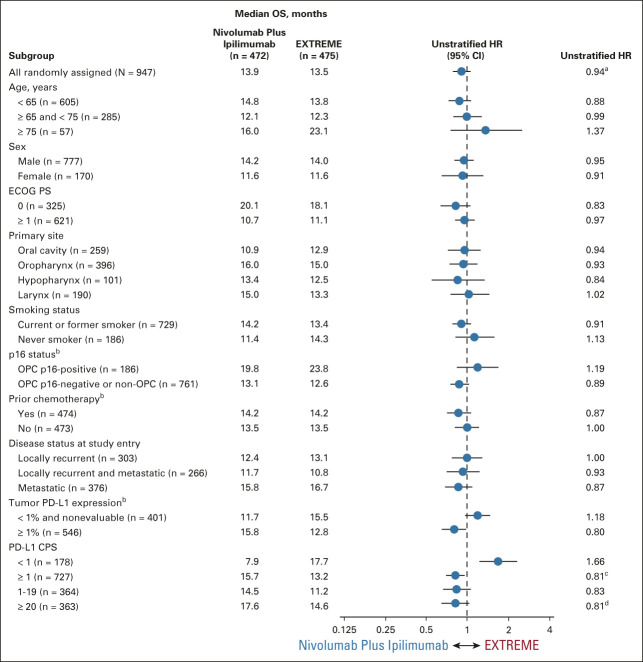
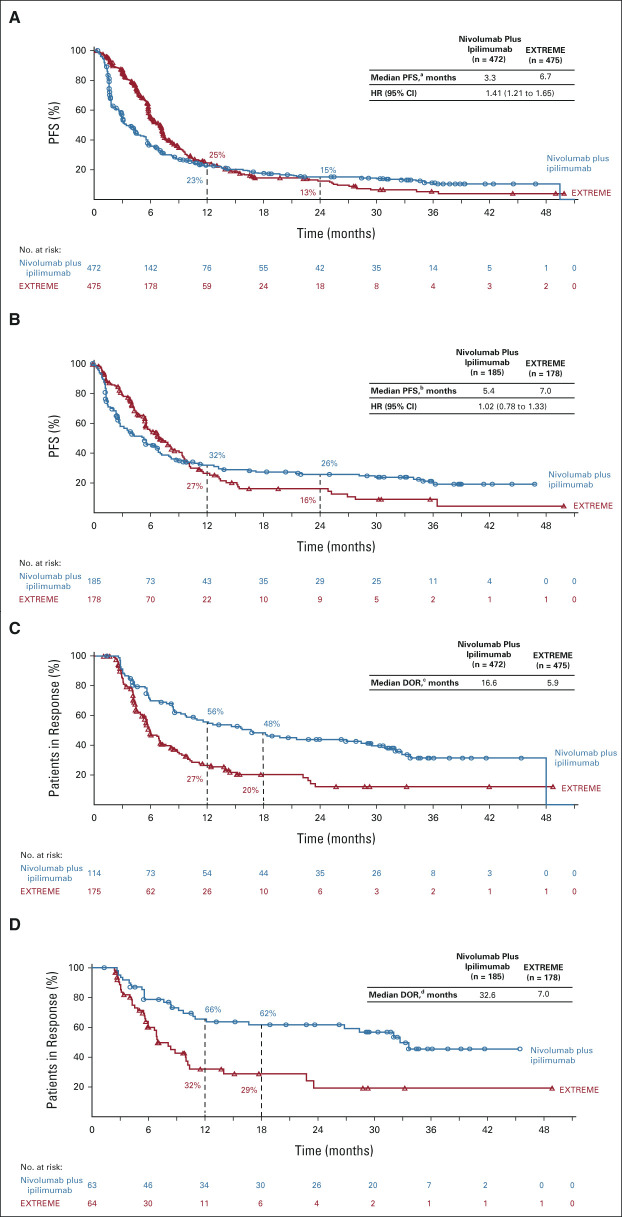
Methods: Patients without prior systemic therapy for R/M SCCHN were randomly assigned 1:1 to nivolumab plus ipilimumab or EXTREME. Primary end points were overall survival (OS) in the all randomly assigned and programmed death-ligand 1 combined positive score (CPS) ≥ 20 populations. Secondary end points included OS in the programmed death-ligand 1 CPS ≥ 1 population, and progression-free survival, objective response rate, and duration of response in the all randomly assigned and CPS ≥ 20 populations.
Results: Among 947 patients randomly assigned, 38.3% had CPS ≥ 20. There were no statistically significant differences in OS with nivolumab plus ipilimumab versus EXTREME in the all randomly assigned (median: 13.9 v 13.5 months; hazard ratio [HR], 0.95; 97.9% CI, 0.80 to 1.13; P = .4951) and CPS ≥ 20 (median: 17.6 v 14.6 months; HR, 0.78; 97.51% CI, 0.59 to 1.03; P = .0469) populations. In patients with CPS ≥ 1, the median OS was 15.7 versus 13.2 months (HR, 0.82; 95% CI, 0.69 to 0.97). Among patients with CPS ≥ 20, the median progression-free survival was 5.4 months (nivolumab plus ipilimumab) versus 7.0 months (EXTREME), objective response rate was 34.1% versus 36.0%, and median duration of response was 32.6 versus 7.0 months. Grade 3/4 treatment-related adverse events occurred in 28.2% of patients treated with nivolumab plus ipilimumab versus 70.7% treated with EXTREME.
Conclusion: CheckMate 651 did not meet its primary end points of OS in the all randomly assigned or CPS ≥ 20 populations. Nivolumab plus ipilimumab showed a favorable safety profile compared with EXTREME. There continues to be a need for new therapies in patients with R/M SCCHN.
Conflict of interest statement
Nivolumab Plus Ipilimumab Versus EXTREME Regimen as First-Line Treatment for Recurrent/Metastatic Squamous Cell Carcinoma of the Head and Neck: The Final Results of CheckMate 651
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Robert I. Haddad
Kevin Harrington
This author is a member of the
Makoto Tahara
Robert L. Ferris
Maura Gillison
This author is an Associate Editor for
Jerome Fayette
Amaury Daste
Bogdan Zurawski
Miren Taberna
Nabil F. Saba
Milena Mak
Andrzej Kawecki
Gustavo Girotto
Caroline Even
Joaquin Gabriel Reinoso Toledo
Alexander Guminski
Urs Müller-Richter
Naomi Kiyota
Mustimbo Roberts
Tariq Aziz Khan
Karen Miller-Moslin
Li Wei
Athanassios Argiris
No other potential conflicts of interest were reported.
Figures
Comment in
-
First-Line Nivolumab Plus Ipilimumab in Recurrent/Metastatic Head and Neck Cancer-What Happened?J Clin Oncol. 2023 Apr 20;41(12):2134-2137. doi: 10.1200/JCO.22.02349. Epub 2023 Mar 6. J Clin Oncol. 2023. PMID: 36877893 No abstract available.
References
-
- Sung H, Ferlay J, Siegel RL, et al. : Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209-249, 2021 - PubMed
-
- Chow LQM: Head and neck cancer. N Engl J Med 382:60-72, 2020 - PubMed
-
- Machiels JP, Rene Leemans C, Golusinski W, et al. : Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO clinical practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 31:1462-1475, 2020 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
