

Superficial Parasternal Intercostal Plane Blocks (SPIB) With Buprenorphine, Magnesium, and Bupivacaine for Management of Pain in Coronary Artery Bypass Grafting
- PMID: 36475128
- PMCID: PMC9719726
- DOI: 10.7759/cureus.30964
Superficial Parasternal Intercostal Plane Blocks (SPIB) With Buprenorphine, Magnesium, and Bupivacaine for Management of Pain in Coronary Artery Bypass Grafting
Abstract
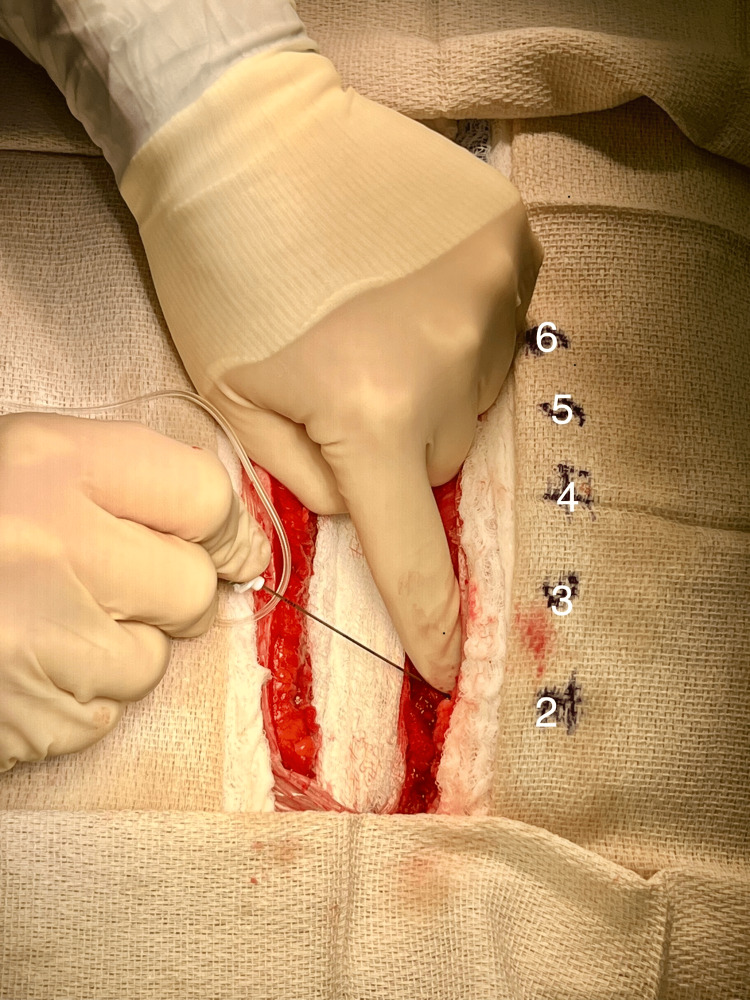
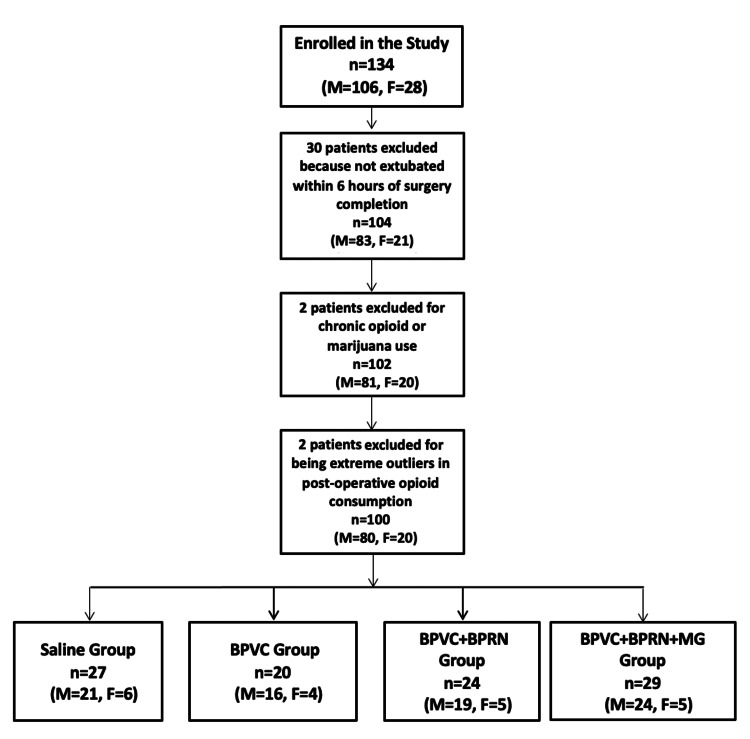
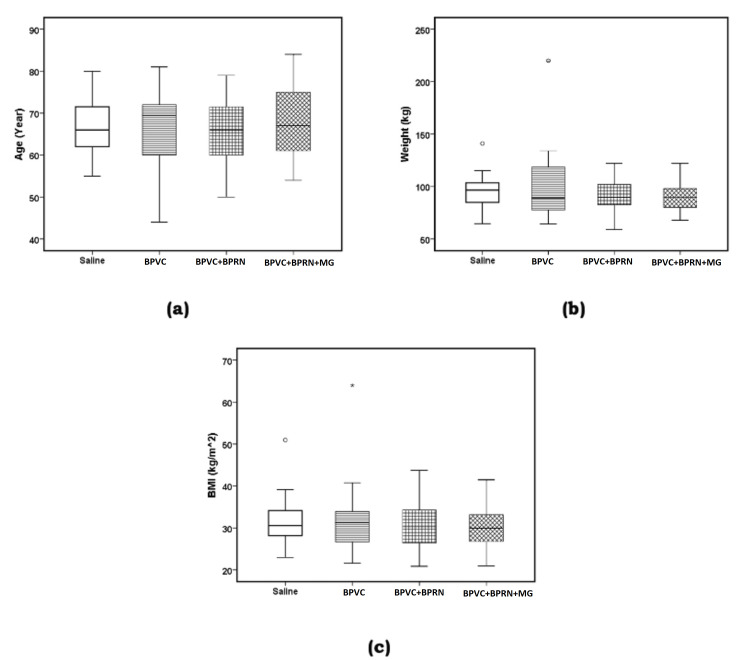
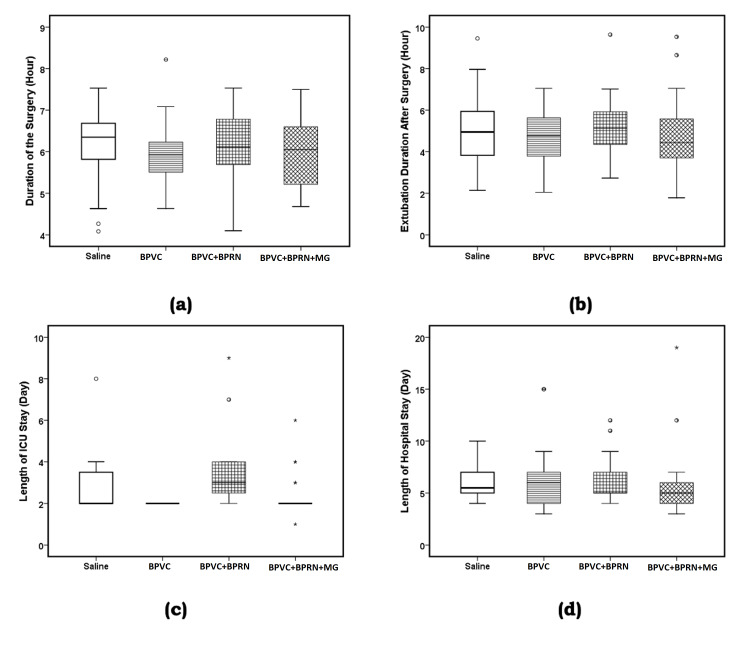
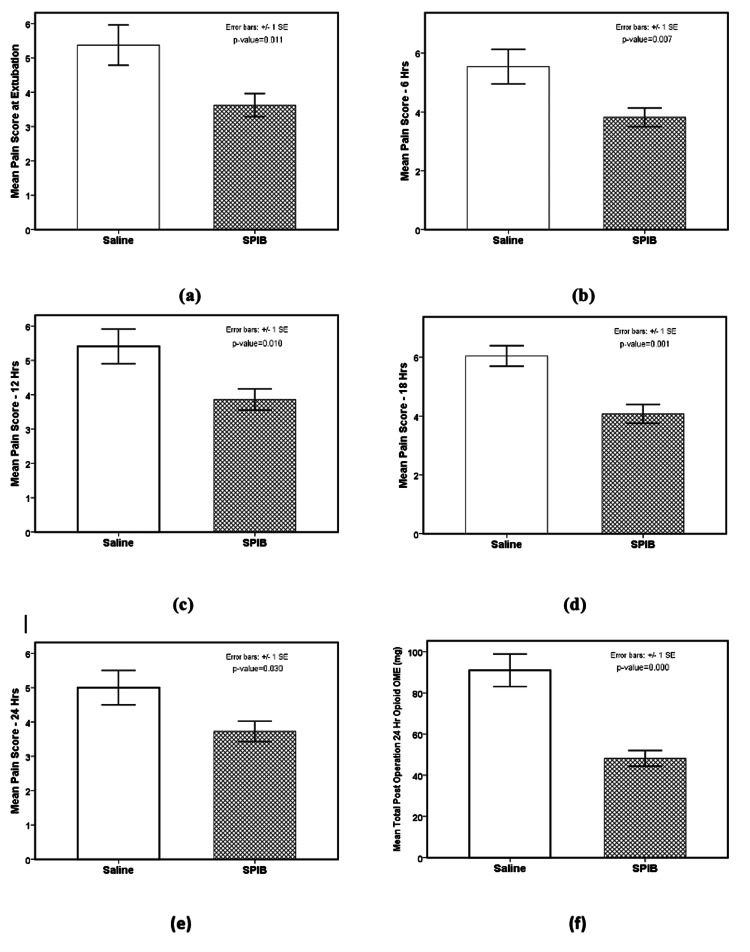
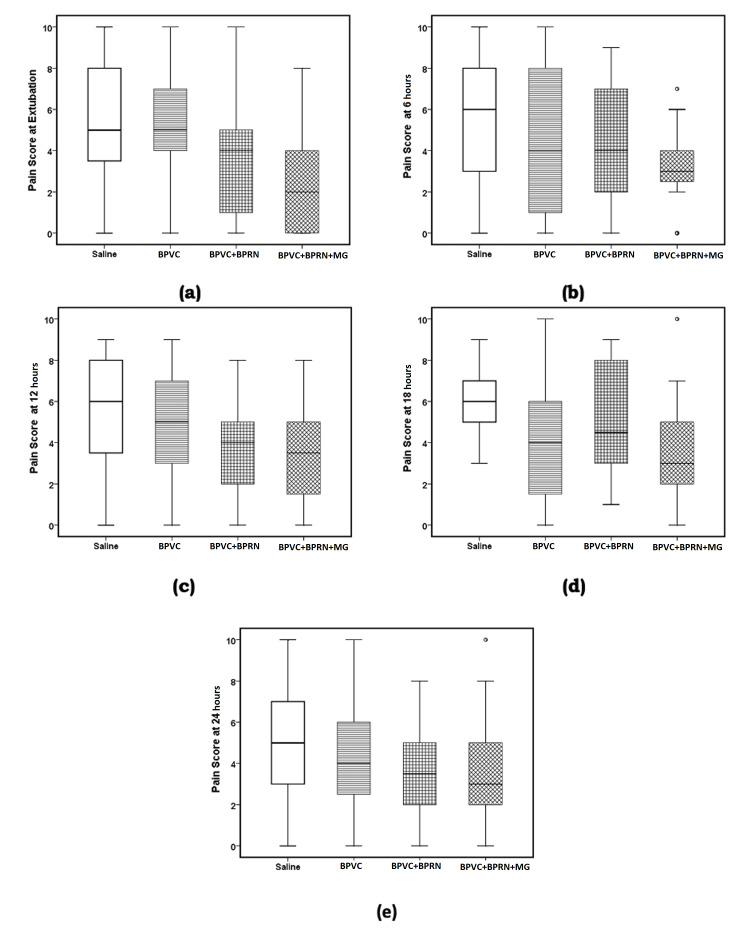
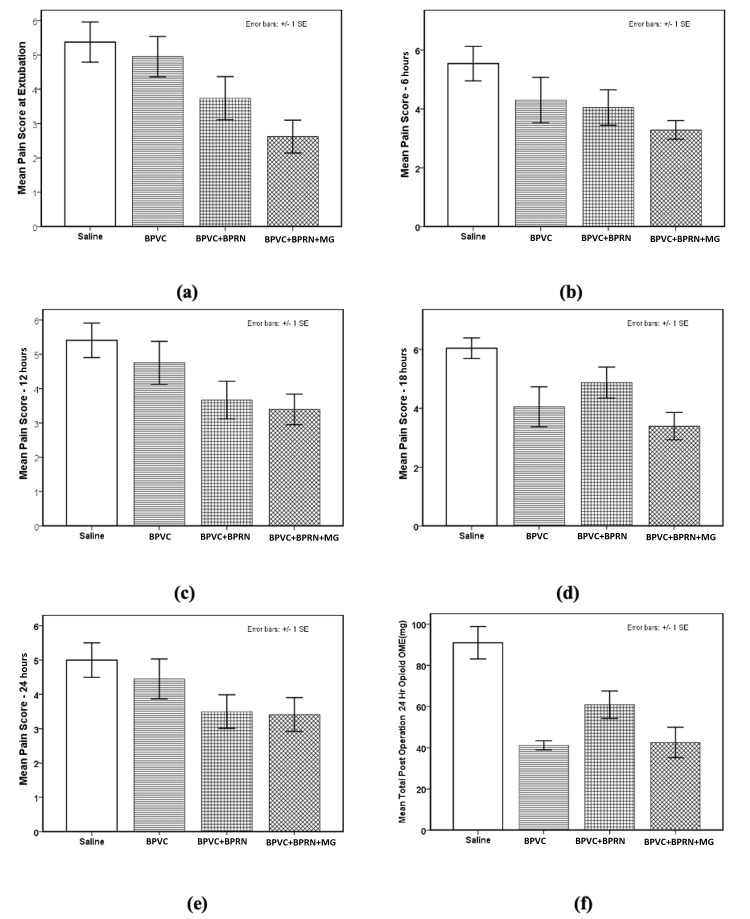
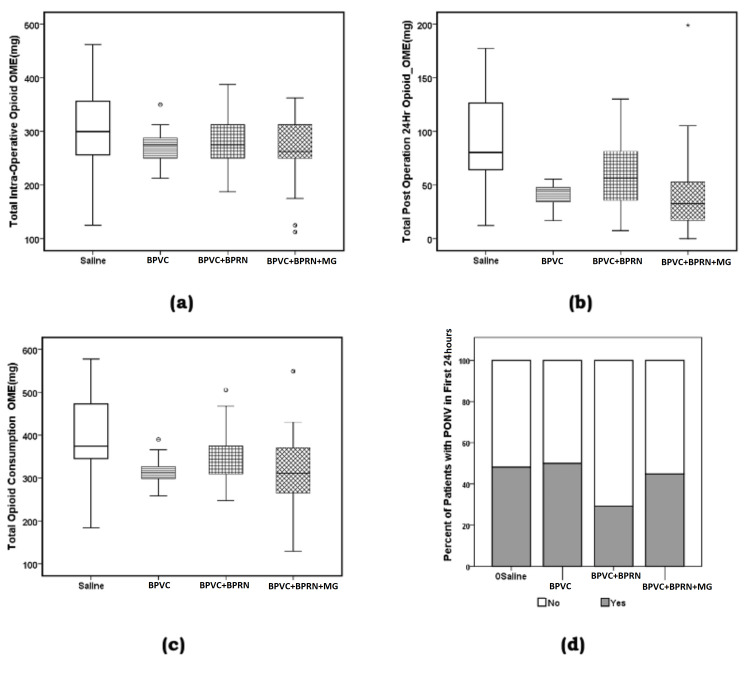
Introduction Management of post-operative pain after cardiac surgery continues to be a challenge; inadequate management of pain can lead to increased morbidity, impaired physical function with potential delay in recovery, increased perioperative and chronic opioid consumption, increased cost of care, and a decreased quality of life. This study aimed to evaluate the effect of adding buprenorphine and magnesium to bupivacaine for superficial parasternal intercostal plane blocks (SPIB) on pain and opioid consumption in the first 24 hours after coronary artery bypass grafting (CABG). Methods Patients undergoing CABG were divided into the following four groups: saline SPIB, SPIB with bupivacaine (BPVC), SPIB with bupivacaine and buprenorphine (BPVC+BPRN), and SPIB with bupivacaine, buprenorphine, and magnesium (BPVC+BPRN+MG). The primary outcomes were pain scores and opioid consumption after SPIB; the secondary outcomes were post-operative nausea and vomiting, time to extubation, and length of stay (LOS) in the intensive care unit and hospital. Results One hundred thirty-four eligible patients undergoing CABG were randomized to either the saline (n=27), BPVC (n=20), BPVC+BPRN (n=24), or BPVC+BPRN+MG (n=29) group. All of the intervention groups combined (BPVC, BPVC+BPRN, and BPVC+BPRN+MG) had decreased pain scores and decreased opioid consumption when compared to the saline group; although not statistically significant, visual analog scale (VAS) scores trended downward at most time points with BPVC versus saline, BPVC+BPRN versus BPVC, and BPVC+BPRN+MG versus BPVC+BPRN. There was no difference among the study groups in the incidence of post-operative nausea and/or vomiting (PONV), time to extubation, hospital LOS, and ICU LOS. Conclusion In this prospective, double-blind, placebo-controlled trial, we found that SPIB with local anesthetic is effective at reducing VAS scores and opioid consumption after CABG. Further study is needed to determine whether the addition of adjuvants can further improve pain control and opioid consumption.
Keywords: buprenorphine; coronary artery bypass grafting; magnesium; post-operative opioid consumption; post-operative pain management; superficial parasternal intercostal block.
Copyright © 2022, Krishnan et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Persistent postoperative pain after cardiac surgery: a systematic review with meta-analysis regarding incidence and pain intensity. Guimarães-Pereira L, Reis P, Abelha F, Azevedo LF, Castro-Lopes JM. Pain. 2017;158:1869–1885. - PubMed
-
- The role of the anesthesiologist in fast-track surgery: from multimodal analgesia to perioperative medical care. White PF, Kehlet H, Neal JM, Schricker T, Carr DB, Carli F. Anesth Analg. 2007;104:1380–1396. - PubMed
-
- Epidural analgesia for cardiac surgery. Svircevic V, Passier MM, Nierich AP, van Dijk D, Kalkman CJ, van der Heijden GJ. Cochrane Database Syst Rev. 2013 - PubMed
LinkOut - more resources
Full Text Sources