

Safety of User-Initiated Intensification of Insulin Delivery Using Cambridge Hybrid Closed-Loop Algorithm
- PMID: 36475908
- PMCID: PMC11307210
- DOI: 10.1177/19322968221141924
Safety of User-Initiated Intensification of Insulin Delivery Using Cambridge Hybrid Closed-Loop Algorithm
Abstract
Objective: Many hybrid closed-loop (HCL) systems struggle to manage unusually high glucose levels as experienced with intercurrent illness or pre-menstrually. Manual correction boluses may be needed, increasing hypoglycemia risk with overcorrection. The Cambridge HCL system includes a user-initiated algorithm intensification mode ("Boost"), activation of which increases automated insulin delivery by approximately 35%, while remaining glucose-responsive. In this analysis, we assessed the safety of "Boost" mode.
Methods: We retrospectively analyzed data from closed-loop studies involving young children (1-7 years, n = 24), children and adolescents (10-17 years, n = 19), adults (≥24 years, n = 13), and older adults (≥60 years, n = 20) with type 1 diabetes. Outcomes were calculated per participant for days with ≥30 minutes of "Boost" use versus days with no "Boost" use. Participants with <10 "Boost" days were excluded. The main outcome was time spent in hypoglycemia <70 and <54 mg/dL.
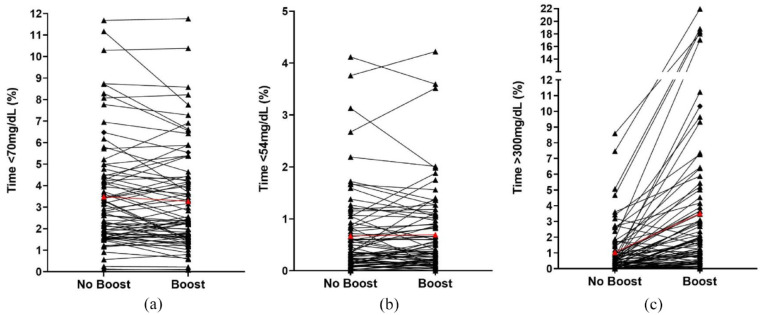
Results: Eight weeks of data for 76 participants were analyzed. There was no difference in time spent <70 and <54 mg/dL between "Boost" days and "non-Boost" days; mean difference: -0.10% (95% confidence interval [CI] -0.28 to 0.07; P = .249) time <70 mg/dL, and 0.03 (-0.04 to 0.09; P = .416) time < 54 mg/dL. Time in significant hyperglycemia >300 mg/dL was 1.39 percentage points (1.01 to 1.77; P < .001) higher on "Boost" days, with higher mean glucose and lower time in target range (P < .001).
Conclusions: Use of an algorithm intensification mode in HCL therapy is safe across all age groups with type 1 diabetes. The higher time in hyperglycemia observed on "Boost" days suggests that users are more likely to use algorithm intensification on days with extreme hyperglycemic excursions.
Keywords: artificial pancreas; automated insulin delivery; closed-loop; hypoglycemia; personalized medicine; type 1 diabetes.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RH reports having received speaker honoraria from Eli Lilly, Dexcom, and Novo Nordisk; receiving license fees from BBraun; patents related to closed-loop; and being director at CamDiab. JW reports receiving speaker honoraria from Ypsomed. YR is a consultant at CamDiab. MEW is a consultant at CamDiab and reports patents related to closed-loop. CKB reports receiving consultancy fees from CamDiab and speaker honoraria from Ypsomed. SH reports speaker and advisory board fees from Dexcom, Medtronic, Sanofi, and Ypsomed; being director at ASK Diabetes Ltd; and receiving consulting/training fees from CamDiab. LB reports receiving research support from Dexcom and CamDiab. REJB reports receiving speaking honoraria from Eli Lilly and Springer Healthcare, and sitting as a voluntary unpaid member of the NovoNordisk UK Foundation Research Selection committee. FMC reports receiving speaker honoraria from Eli Lilly, Dexcom, and Novo Nordisk and Insulet, and consultancy fees from Abbott Diabetes Care. EF-R reports having received speaker honoraria from Eli Lilly and Novo Nordisk, serving on advisory boards for Eli Lilly and Sanofi. MLE is a clinical triallist with or has served on advisory boards or received speakers or writers fees from Medtronic, Dexcom, Abbott Diabetes Care, Roche, AstraZeneca, Novo Nordisk, Eli Lilly, Zucara, Pila Pharma, and Imcyse Pharma. SEH has received speaker honoraria by Eli Lilly, Vertex, Minimed Medtronic, Insulet, Ypsomed, and Sanofi. TMK reports having received speaker honoraria from Eli Lilly and Novo. LL has received personal fees from Abbott Diabetes Care, Dexcom, Insulet, Medtronic, Novo Nordisk, Sanofi, and Diabetes Care. JKM is a member on the advisory board of Boehringer Ingelheim, Becton-Dickinson, Eli Lilly, Medtronic, Prediktor A/S, Roche Diabetes Care, and Sanofi-Aventis, and received speaker honoraria from Abbott Diabetes Care, AstraZeneca, Becton-Dickinson, Dexcom, Eli Lilly, Mercke Sharp & Dohme, NovoNordisk, Roche Diabetes Care, Sanofi, Servier, and Ypsomed. TR reports receiving speaker honoraria from Novo Nordisk and consultancy fees from Abbott Diabetes Care. HT reports receiving research support from Dexcom and speaker honoraria from Eli Lilly. MT reports having received speaker honoraria from Eli Lilly, Novo Nordisk, and Medtronic and advisory board fees from Abbott Diabetes Care. BR-M has received speaker honoraria from Abbott Diabetes Care, Eli Lilly, Medtronic, Novo Nordisk, Roche Diabetes Care, Sanofi, and Menarini and has been on the advisory boards of Eli Lilly, Roche Diabetes Care, and Abbott Diabetes Care. CdB has received speaker honoraria from Minimed Medtronic, and has been member of their European Psychology and e-learning Advisory Board. JMA reports training fees from CamDiab. DE, WMM, PN, TP, AG, AT, KD, and NT have no disclosures.
Figures
References
-
- Ware J, Allen JM, Boughton CK, et al. Randomized trial of closed-loop control in very young children with type 1 diabetes. N Engl J Med. 2022;386(3):209-219. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
