

The Human Respiratory Microbiome: Current Understandings and Future Directions
- PMID: 36476129
- PMCID: PMC9989478
- DOI: 10.1165/rcmb.2022-0208TR
The Human Respiratory Microbiome: Current Understandings and Future Directions
Abstract
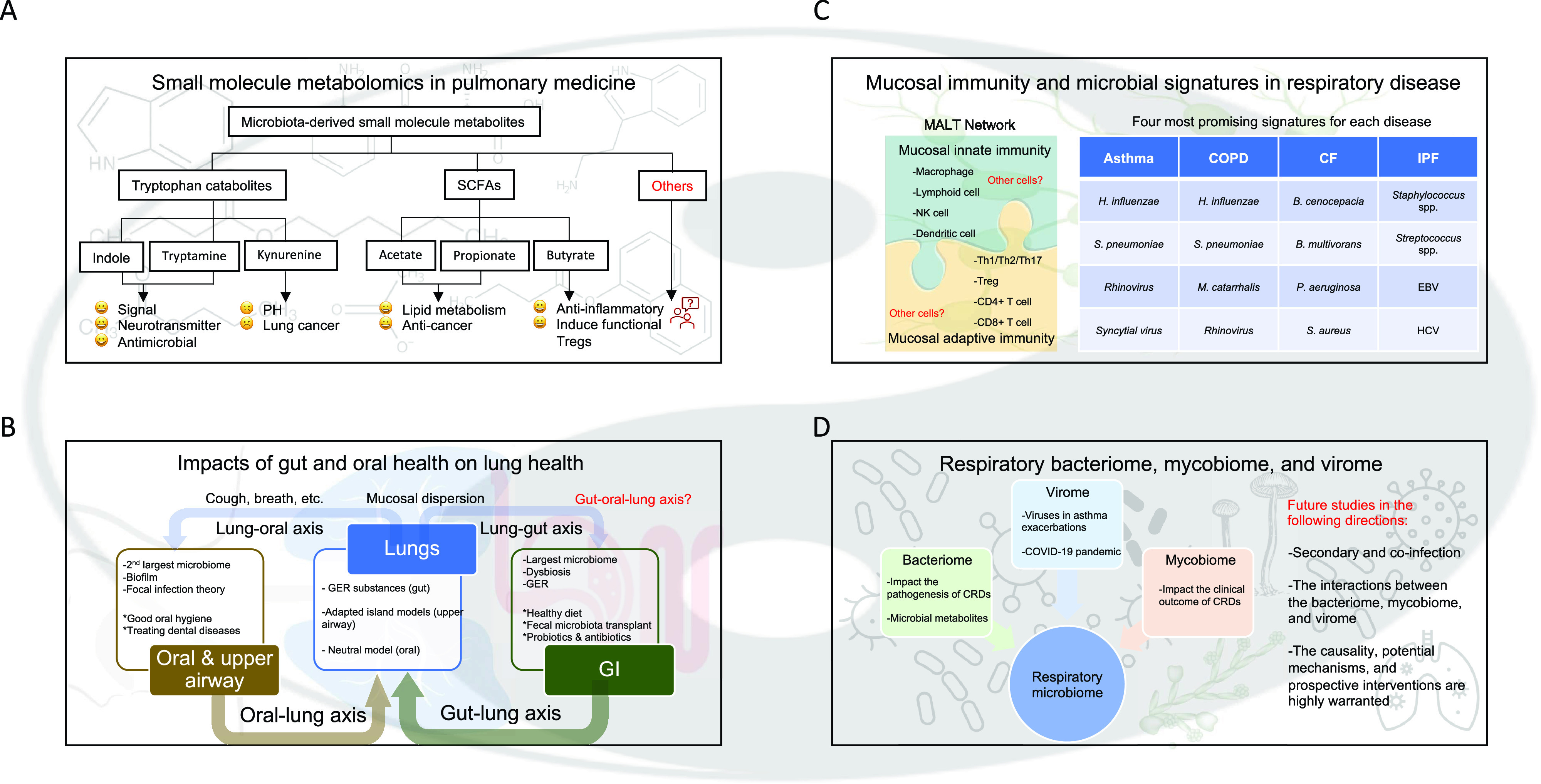
Microorganisms colonize the human body. The lungs and respiratory tract, previously believed to be sterile, harbor diverse microbial communities and the genomes of bacteria (bacteriome), viruses (virome), and fungi (mycobiome). Recent advances in amplicon and shotgun metagenomic sequencing technologies and data-analyzing methods have greatly aided the identification and characterization of microbial populations from airways. The respiratory microbiome has been shown to play roles in human health and disease and is an area of rapidly emerging interest in pulmonary medicine. In this review, we provide updated information in the field by focusing on four lung conditions, including asthma, chronic obstructive pulmonary disease, cystic fibrosis, and idiopathic pulmonary fibrosis. We evaluate gut, oral, and upper airway microbiomes and how they contribute to lower airway flora. The discussion is followed by a systematic review of the lower airway microbiome in health and disease. We conclude with promising research avenues and implications for evolving therapeutics.
Keywords: microbial metabolites; microbiome; mucus; respiratory diseases; therapeutics.
Figures

References
-
- Pugin J, Auckenthaler R, Mili N, Janssens J-P, Lew PD, Suter PM. Diagnosis of ventilator-associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid. Am Rev Respir Dis . 1991;143:1121–1129. - PubMed
-
- Meyer KC, Raghu G. Bronchoalveolar lavage for the evaluation of interstitial lung disease: is it clinically useful? Eur Respir J . 2011;38:761–769. - PubMed
-
- Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, Bønnelykke K, et al. Childhood asthma after bacterial colonization of the airway in neonates. N Engl J Med . 2007;357:1487–1495. - PubMed
-
- Hill AT, Campbell EJ, Hill SL, Bayley DL, Stockley RA. Association between airway bacterial load and markers of airway inflammation in patients with stable chronic bronchitis. Am J Med . 2000;109:288–295. - PubMed
