

Predicting the risk of acute kidney injury after cardiopulmonary bypass: development and assessment of a new predictive nomogram
- PMID: 36476178
- PMCID: PMC9727998
- DOI: 10.1186/s12871-022-01925-w
Predicting the risk of acute kidney injury after cardiopulmonary bypass: development and assessment of a new predictive nomogram
Abstract
Background: Acute kidney injury (AKI) is a common and severe complication of cardiac surgery with cardiopulmonary bypass (CPB). This study aimed to establish a model to predict the probability of postoperative AKI in patients undergoing cardiac surgery with CPB.
Methods: We conducted a retrospective, multicenter study to analyze 1082 patients undergoing cardiac surgery under CPB. The least absolute shrinkage and selection operator regression model was used to optimize feature selection for the AKI model. Multivariable logistic regression analysis was applied to build a prediction model incorporating the feature selected in the previously mentioned model. Finally, we used multiple methods to evaluate the accuracy and clinical applicability of the model.
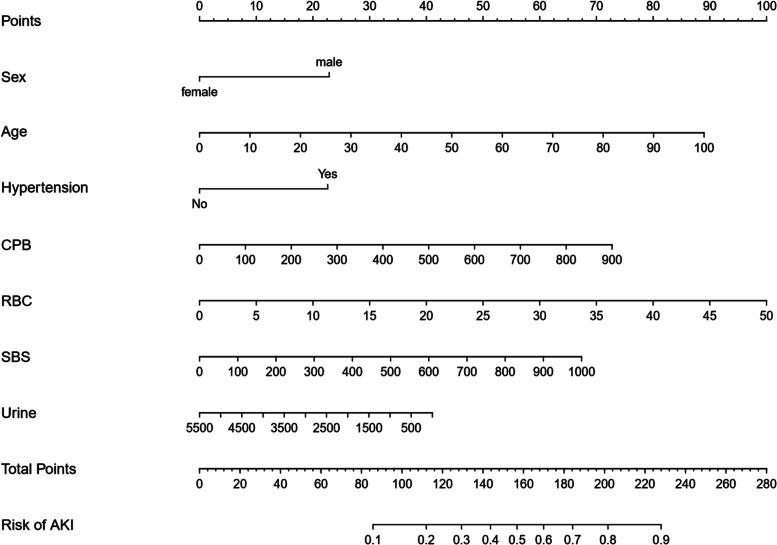
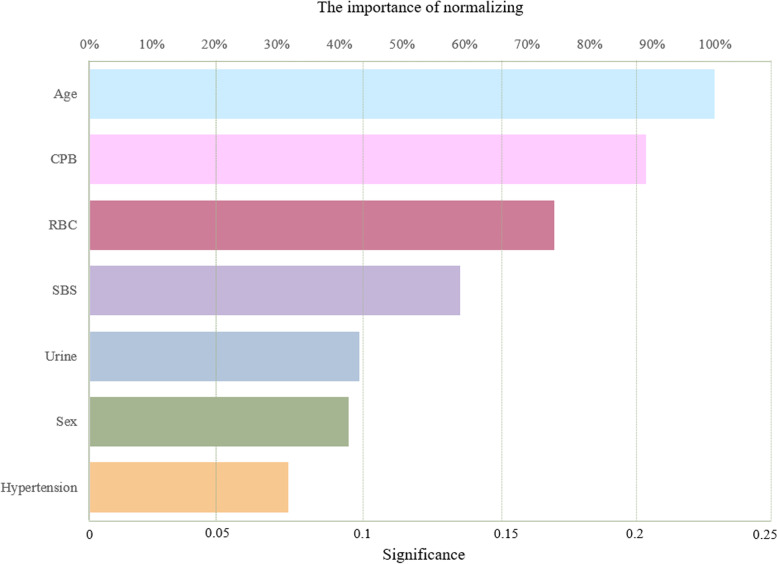
Results: Age, gender, hypertension, CPB duration, intraoperative 5% bicarbonate solution and red blood cell transfusion, urine volume were identified as important factors. Then, these risk factors were created into nomogram to predict the incidence of AKI after cardiac surgery under CPB.
Conclusion: We developed a nomogram to predict the incidence of AKI after cardiac surgery. This model can be used as a reference tool for evaluating early medical intervention to prevent postoperative AKI.
Keywords: Acute kidney injury; Cardiac surgery; Cardiopulmonary bypass; Nomogram; Prevention.
© 2022. The Author(s).
Conflict of interest statement
There is no conflict of interest involved in this study.
Figures




Similar articles
-
Development and Validation of a Nomogram for Predicting Acute Kidney Injury in Pediatric Patients Undergoing Cardiac Surgery.Pediatr Cardiol. 2025 Feb;46(2):305-311. doi: 10.1007/s00246-023-03392-7. Epub 2024 Jan 13. Pediatr Cardiol. 2025. PMID: 38217691
-
A model for predicting AKI after cardiopulmonary bypass surgery in Chinese patients with normal preoperative renal function.BMC Surg. 2024 Dec 2;24(1):383. doi: 10.1186/s12893-024-02683-x. BMC Surg. 2024. PMID: 39617905 Free PMC article.
-
Urine Output During Cardiopulmonary Bypass Predicts Acute Kidney Injury After Cardiac Surgery: A Single-Center Retrospective Analysis.Medicine (Baltimore). 2016 May;95(22):e3757. doi: 10.1097/MD.0000000000003757. Medicine (Baltimore). 2016. PMID: 27258505 Free PMC article.
-
Cardiac surgery-associated acute kidney injury.Blood Purif. 2014;37 Suppl 2:34-50. doi: 10.1159/000361062. Epub 2014 Jul 31. Blood Purif. 2014. PMID: 25196567 Review.
-
Association between postoperative acute kidney injury and duration of cardiopulmonary bypass: a meta-analysis.J Cardiothorac Vasc Anesth. 2012 Feb;26(1):64-9. doi: 10.1053/j.jvca.2011.07.007. Epub 2011 Sep 15. J Cardiothorac Vasc Anesth. 2012. PMID: 21924633
Cited by
-
A systematic review of cardiac surgery clinical prediction models that include intra-operative variables.Perfusion. 2025 Mar;40(2):328-342. doi: 10.1177/02676591241237758. Epub 2024 Apr 22. Perfusion. 2025. PMID: 38649154 Free PMC article.
-
Development and Validation of a Nomogram for Predicting Acute Kidney Injury in Pediatric Patients Undergoing Cardiac Surgery.Pediatr Cardiol. 2025 Feb;46(2):305-311. doi: 10.1007/s00246-023-03392-7. Epub 2024 Jan 13. Pediatr Cardiol. 2025. PMID: 38217691
-
A model for predicting AKI after cardiopulmonary bypass surgery in Chinese patients with normal preoperative renal function.BMC Surg. 2024 Dec 2;24(1):383. doi: 10.1186/s12893-024-02683-x. BMC Surg. 2024. PMID: 39617905 Free PMC article.
-
Machine learning for risk prediction of acute kidney injury in patients with diabetes mellitus combined with heart failure during hospitalization.Sci Rep. 2025 Mar 28;15(1):10728. doi: 10.1038/s41598-025-87268-1. Sci Rep. 2025. PMID: 40155666 Free PMC article.
References
-
- Kališnik JM, Hrovat E, Hrastovec A, Žibert J, Jerin A, Skitek M, Santarpino G, Klokocovnik T. Creatinine, neutrophil gelatinase-associated lipocalin, and cystatin C in determining acute kidney injury after heart operations using cardiopulmonary bypass. Artif Organs. 2017;41(5):481–9. doi: 10.1111/aor.12779. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
