

Prediction of oxygen requirement in patients with COVID-19 using a pre-trained chest radiograph xAI model: efficient development of auditable risk prediction models via a fine-tuning approach
- PMID: 36476724
- PMCID: PMC9729627
- DOI: 10.1038/s41598-022-24721-5
Prediction of oxygen requirement in patients with COVID-19 using a pre-trained chest radiograph xAI model: efficient development of auditable risk prediction models via a fine-tuning approach
Erratum in
-
Author Correction: Prediction of oxygen requirement in patients with COVID-19 using a pre-trained chest radiograph xAI model: efficient development of auditable risk prediction models via a fine-tuning approach.Sci Rep. 2023 Mar 15;13(1):4296. doi: 10.1038/s41598-023-31333-0. Sci Rep. 2023. PMID: 36922618 Free PMC article. No abstract available.
Abstract
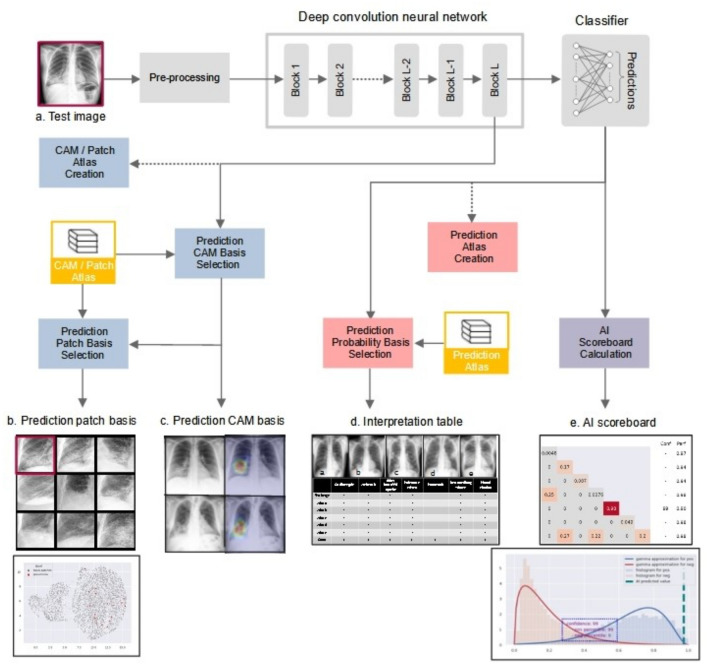
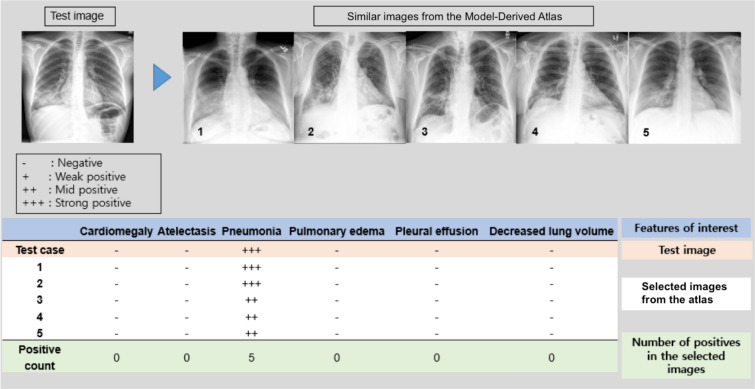
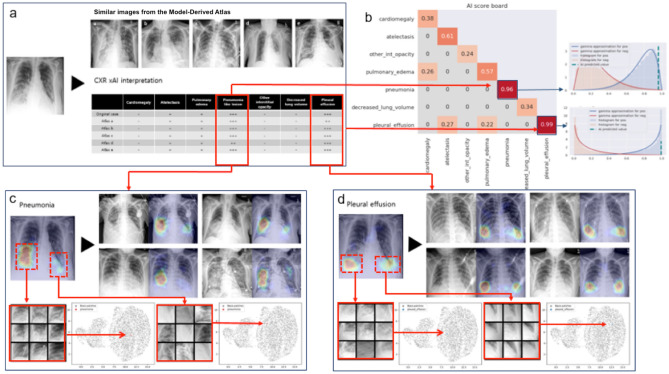
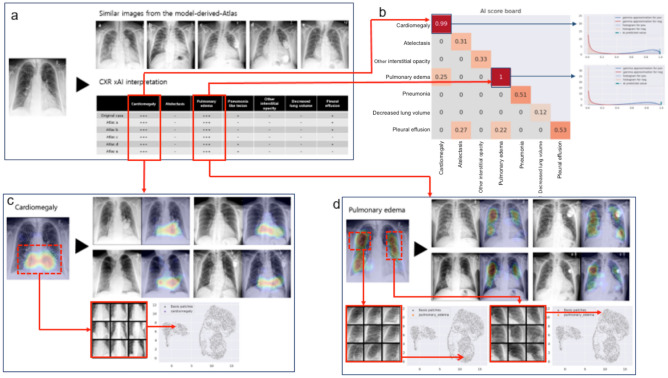
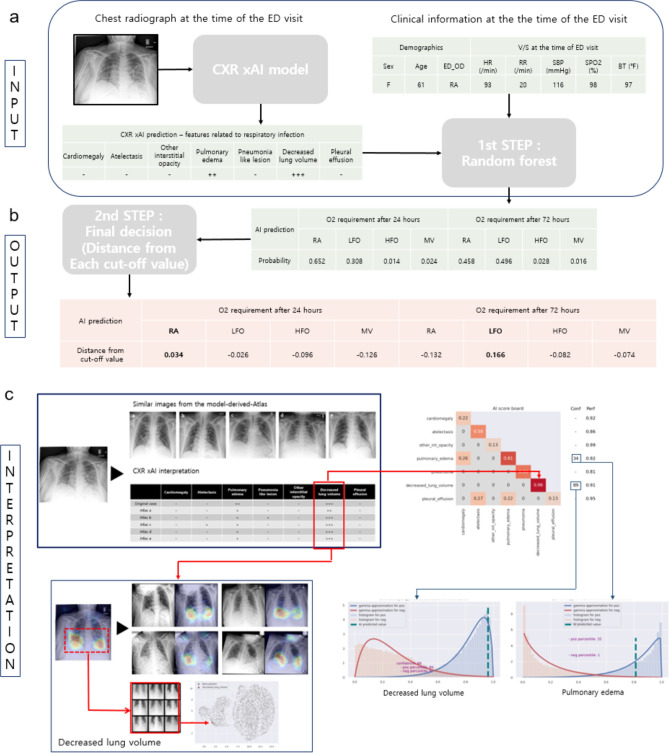
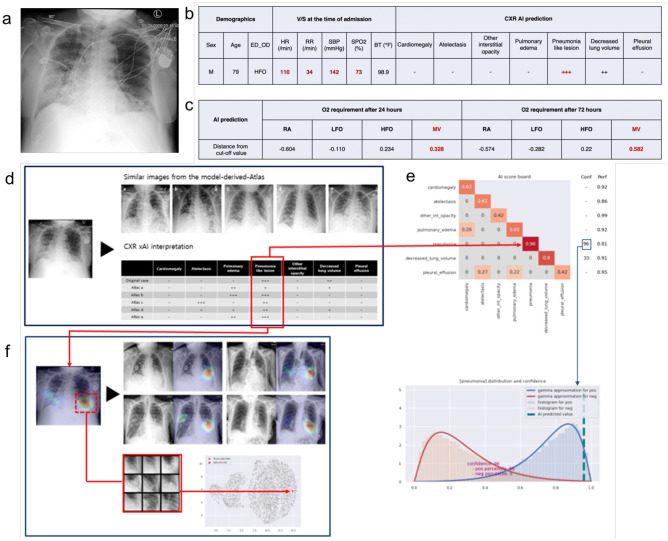
Risk prediction requires comprehensive integration of clinical information and concurrent radiological findings. We present an upgraded chest radiograph (CXR) explainable artificial intelligence (xAI) model, which was trained on 241,723 well-annotated CXRs obtained prior to the onset of the COVID-19 pandemic. Mean area under the receiver operating characteristic curve (AUROC) for detection of 20 radiographic features was 0.955 (95% CI 0.938-0.955) on PA view and 0.909 (95% CI 0.890-0.925) on AP view. Coexistent and correlated radiographic findings are displayed in an interpretation table, and calibrated classifier confidence is displayed on an AI scoreboard. Retrieval of similar feature patches and comparable CXRs from a Model-Derived Atlas provides justification for model predictions. To demonstrate the feasibility of a fine-tuning approach for efficient and scalable development of xAI risk prediction models, we applied our CXR xAI model, in combination with clinical information, to predict oxygen requirement in COVID-19 patients. Prediction accuracy for high flow oxygen (HFO) and mechanical ventilation (MV) was 0.953 and 0.934 at 24 h and 0.932 and 0.836 at 72 h from the time of emergency department (ED) admission, respectively. Our CXR xAI model is auditable and captures key pathophysiological manifestations of cardiorespiratory diseases and cardiothoracic comorbidities. This model can be efficiently and broadly applied via a fine-tuning approach to provide fully automated risk and outcome predictions in various clinical scenarios in real-world practice.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
