

Association of In Utero Antipsychotic Medication Exposure With Risk of Congenital Malformations in Nordic Countries and the US
- PMID: 36477338
- PMCID: PMC9856848
- DOI: 10.1001/jamapsychiatry.2022.4109
Association of In Utero Antipsychotic Medication Exposure With Risk of Congenital Malformations in Nordic Countries and the US
Abstract
Importance: Psychiatric disorders are common among female individuals of reproductive age. While antipsychotic medication use is increasing, the safety of such medications in pregnancy is an area with large evidence gaps.
Objective: To evaluate the risk of first-trimester antipsychotic exposure with respect to congenital malformations, focusing on individual drugs and specific malformation subtypes.
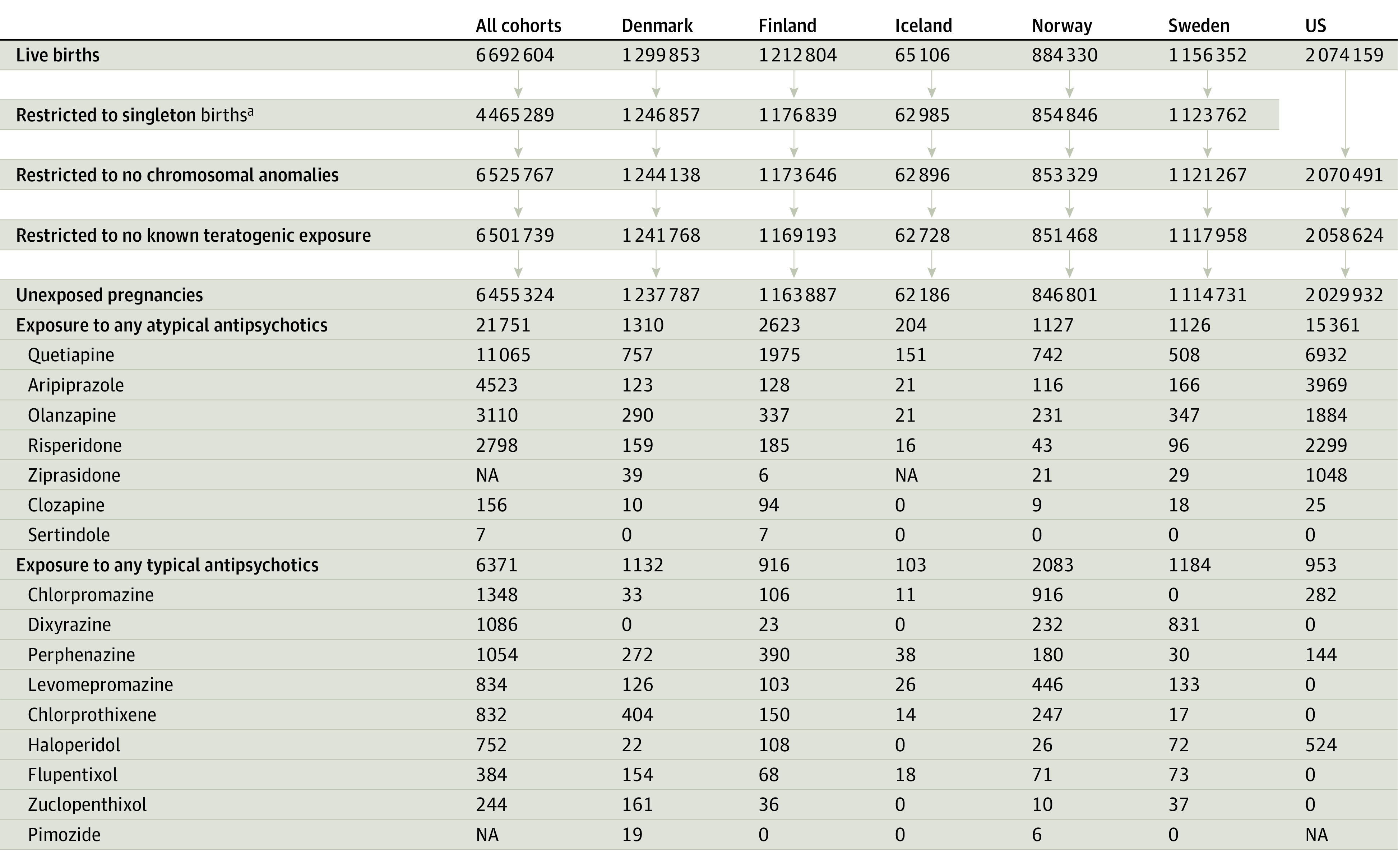
Design, setting, and participants: This cohort study used data from nationwide health registers from the 5 Nordic countries and the US and spanned 1996 to 2018. The Nordic cohort included all pregnancies resulting in singleton live-born infants, and the US cohort consisted of publicly insured mothers linked to their live-born infants nested in the nationwide Medicaid Analytic eXtract. Data were analyzed from November 2020 to April 2022.
Exposures: One or more first-trimester dispensing of any atypical, any typical, and individual antipsychotic drugs.
Main outcomes and measures: Any major congenital malformation and specific malformation subtypes previously suggested to be associated with antipsychotic exposure in utero: cardiovascular malformations, oral clefts, neural tube defects, hip dysplasia, limb reduction defects, anorectal atresia/stenosis, gastroschisis, hydrocephalus, other specific brain anomalies, and esophageal disorders. Propensity score stratification was used to control for potential confounders. Pooled adjusted estimates were calculated using indirect standardization.
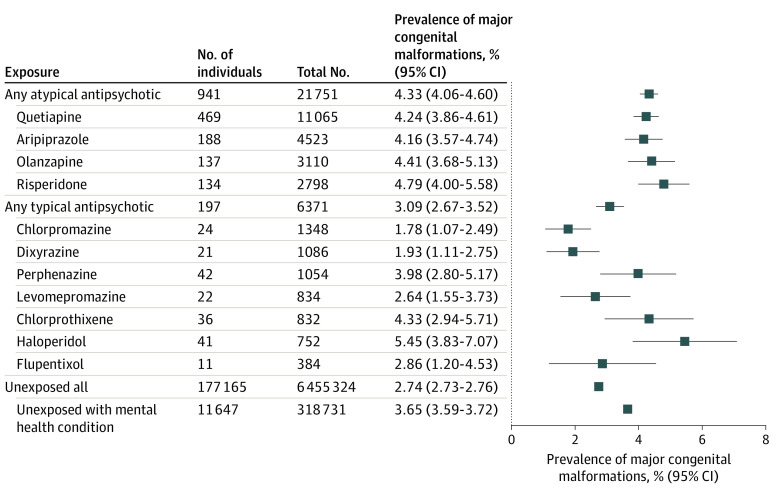
Results: A total of 6 455 324 unexposed mothers (mean maternal age range across countries: 24-31 years), 21 751 mothers exposed to atypical antipsychotic drugs (mean age range, 26-31 years), and 6371 mothers exposed to typical antipsychotic drugs (mean age range, 27-32 years) were included in the study cohort. Prevalence of any major malformation was 2.7% (95% CI, 2.7%-2.8%) in unexposed infants, 4.3% (95% CI, 4.1%-4.6%) in infants with atypical antipsychotic drug exposure, and 3.1% (95% CI, 2.7%-3.5%) in infants with typical antipsychotic drug exposure in utero. Among the most prevalent exposure-outcome combinations, adjusted relative risks (aRR) were generally close to the null. One exception was olanzapine exposure and oral cleft (aRR, 2.1 [95% CI, 1.1-4.3]); however, estimates varied across sensitivity analyses. Among moderately prevalent combinations, increased risks were observed for gastroschisis and other specific brain anomalies after atypical antipsychotic exposure (aRR, 1.5 [95% CI, 0.8-2.6] and 1.9 [95% CI, 1.1-3.0]) and for cardiac malformations after chlorprothixene exposure (aRR, 1.6 [95% CI, 1.0-2.7]). While the association direction was consistent across sensitivity analyses, confidence intervals were wide, prohibiting firm conclusions.
Conclusions and relevance: In this study, considering the evidence from primary and sensitivity analyses and inevitable statistical noise for very rare exposure-outcome combinations, in utero antipsychotic exposure generally was not meaningfully associated with an increased risk of malformations. The observed increased risks of oral clefts associated with olanzapine, gastroschisis, and other specific brain anomalies with atypical antipsychotics and cardiac malformations with chlorprothixene requires confirmation as evidence continues to accumulate.
Conflict of interest statement
Figures


References
-
- Nemeroff CB. Use of atypical antipsychotics in refractory depression and anxiety. J Clin Psychiatry. 2005;66(suppl 8):13-21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
