

Hypo-osmolar rectal douche tenofovir formulation prevents simian/human immunodeficiency virus acquisition in macaques
- PMID: 36477356
- PMCID: PMC9746910
- DOI: 10.1172/jci.insight.161577
Hypo-osmolar rectal douche tenofovir formulation prevents simian/human immunodeficiency virus acquisition in macaques
Abstract
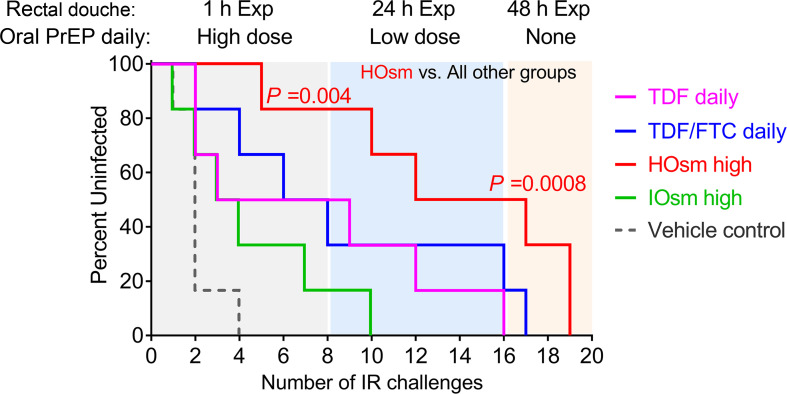
In spite of the rollout of oral pre-exposure prophylaxis (PrEP), the rate of new HIV infections remains a major health crisis. In the United States, new infections occur predominantly in men having sex with men (MSM) in rural settings where access to PrEP can be limited. As an alternative congruent with MSM sexual behavior, we have optimized and tested tenofovir (TFV) and analog-based iso-osmolar and hypo-osmolar (HOsm) rectal douches for efficacy against rectal simian/human immunodeficiency virus (SHIV) infection of macaques. Single TFV HOsm high-dose douches achieved peak plasma TFV levels similar to daily oral PrEP, while other formulations yielded lower concentrations. Rectal tissue TFV-diphosphate (TFV-DP) concentrations at the portal of virus entry, however, were markedly higher after HOsm douching than daily oral PrEP. Repeated douches led to significantly higher plasma TFV and higher TFV-DP concentrations in rectal tissue at 24 hours compared with single douches, without detectable mucosal or systemic toxicity. Using stringent repeated intrarectal SHIV exposures, single HOsm high-dose douches delivered greater protection from virus acquisition for more than 24 hours compared with oral PrEP. Our results demonstrate a rapid delivery of protective TFV doses to the rectal portal of virus entry as a potential low-cost and safe PrEP alternative.
Keywords: AIDS/HIV; Pharmacology; Virology.
Conflict of interest statement
Figures





Similar articles
-
Hypo-osmolar Formulation of Tenofovir (TFV) Enema Promotes Uptake and Metabolism of TFV in Tissues, Leading to Prevention of SHIV/SIV Infection.Antimicrob Agents Chemother. 2017 Dec 21;62(1):e01644-17. doi: 10.1128/AAC.01644-17. Print 2018 Jan. Antimicrob Agents Chemother. 2017. PMID: 29084755 Free PMC article.
-
Development of rectal enema as microbicide (DREAM): Preclinical progressive selection of a tenofovir prodrug enema.Eur J Pharm Biopharm. 2019 May;138:23-29. doi: 10.1016/j.ejpb.2018.05.030. Epub 2018 May 24. Eur J Pharm Biopharm. 2019. PMID: 29802984 Free PMC article.
-
Prevention of vaginal SHIV transmission in macaques by a coitally-dependent Truvada regimen.PLoS One. 2012;7(12):e50632. doi: 10.1371/journal.pone.0050632. Epub 2012 Dec 4. PLoS One. 2012. PMID: 23226529 Free PMC article.
-
The effectiveness of tenofovir-based pre-exposure prophylaxis for prevention of HIV acquisition among sub-Saharan African women at high risk: a systematic review.Pan Afr Med J. 2021 Mar 26;38:308. doi: 10.11604/pamj.2021.38.308.26014. eCollection 2021. Pan Afr Med J. 2021. PMID: 34178226 Free PMC article.
-
Animal models of antiretroviral prophylaxis for HIV prevention.Curr Opin HIV AIDS. 2012 Nov;7(6):505-13. doi: 10.1097/COH.0b013e328358e484. Curr Opin HIV AIDS. 2012. PMID: 22964889 Review.
Cited by
-
The Global Impact of Diversifying PrEP Options: Results of an International Discrete Choice Experiment of Existing and Potential PrEP Strategies with Gay and Bisexual Men and Physicians.AIDS Res Hum Retroviruses. 2024 Oct;40(10):591-605. doi: 10.1089/AID.2023.0120. Epub 2024 May 28. AIDS Res Hum Retroviruses. 2024. PMID: 38753738
-
Tenofovir Douche as HIV Preexposure Prophylaxis for Receptive Anal Intercourse: Safety, Acceptability, Pharmacokinetics, and Pharmacodynamics (DREAM 01).J Infect Dis. 2024 Apr 12;229(4):1131-1140. doi: 10.1093/infdis/jiad535. J Infect Dis. 2024. PMID: 38019657 Free PMC article. Clinical Trial.
References
-
- UNAIDS. Global HIV & AIDS statistics Fact sheet: 2021. https://www.unaids.org/en/resources/fact-sheet Accessed October 21, 2022.
-
- Centers for Disease Control and Prevention. HIV Surveillance Report. http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html Accessed October 21, 2022.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
