

Differentiating between bacterial and viral infections by estimated CRP velocity
- PMID: 36477474
- PMCID: PMC9728869
- DOI: 10.1371/journal.pone.0277401
Differentiating between bacterial and viral infections by estimated CRP velocity
Abstract
Purpose: Differentiating between acute viral and bacterial infection is challenging due to the similarity in symptom presentation. Blood tests can assist in the diagnosis, but they reflect the immediate status and fail to consider the dynamics of an inflammatory response with time since symptom onset. We applied estimated C-reactive protein (CRP) velocity (eCRPv), as derived from the admission CRP level divided by time from symptom onset, in order to better distinguish between viral and bacterial infections.
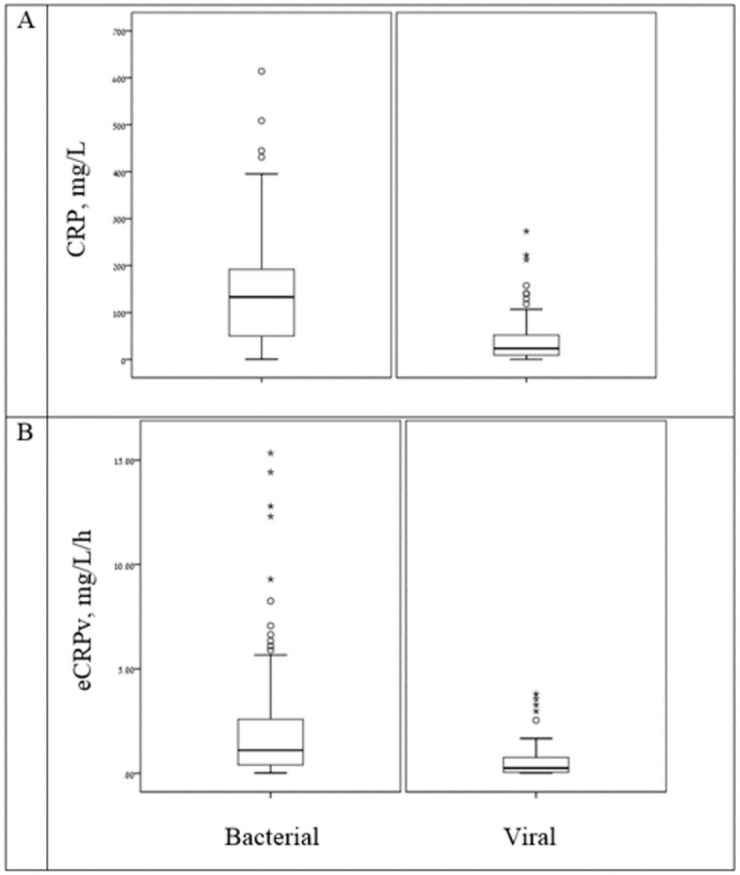
Methods: This cross-sectional study included patients admitted to the emergency department with a confirmed viral (n = 83) or bacterial (n = 181) infection. eCRPv was defined as the ratio between the absolute CRP level upon admission to time from symptom onset (in hours). Absolute CRP and eCRPv values were compared between the 3 groups.
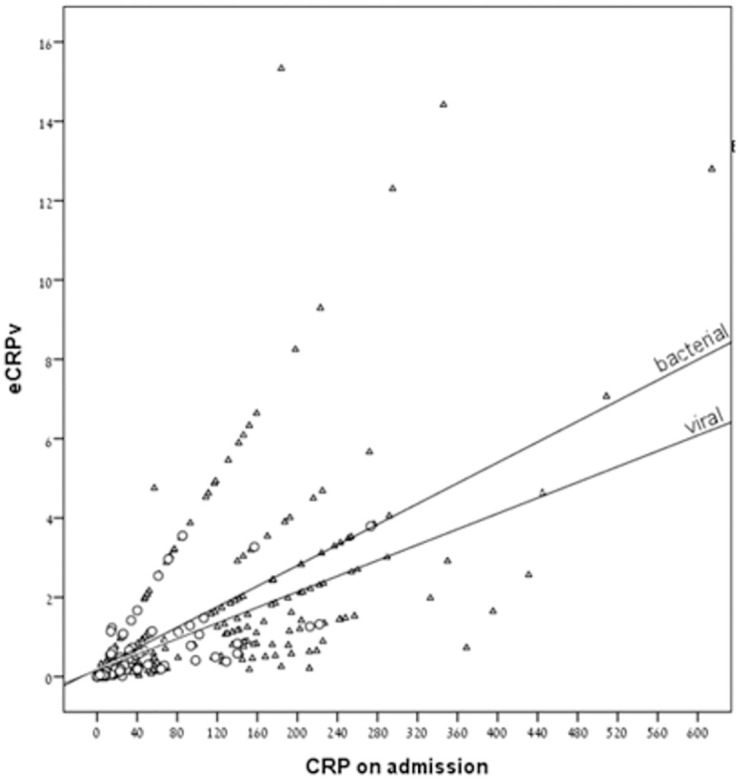
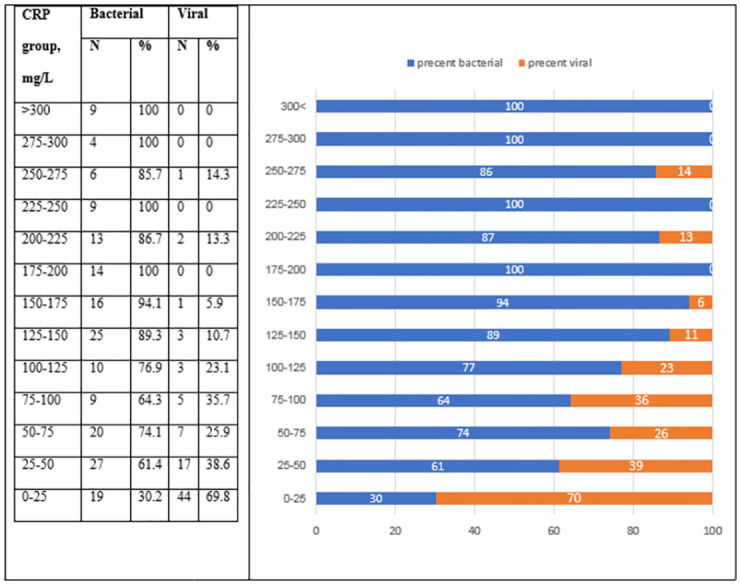
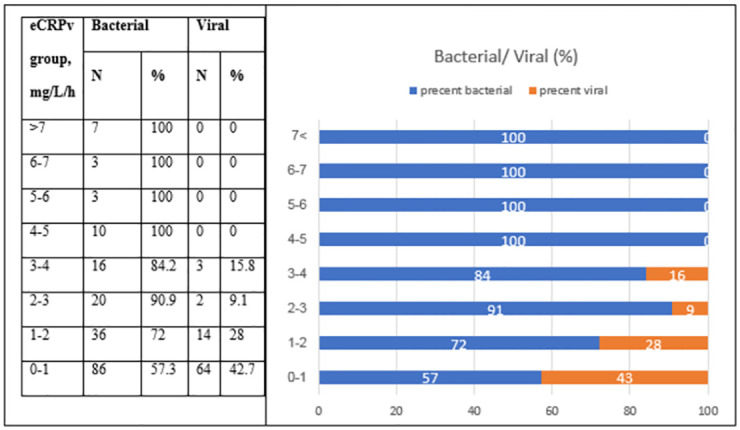
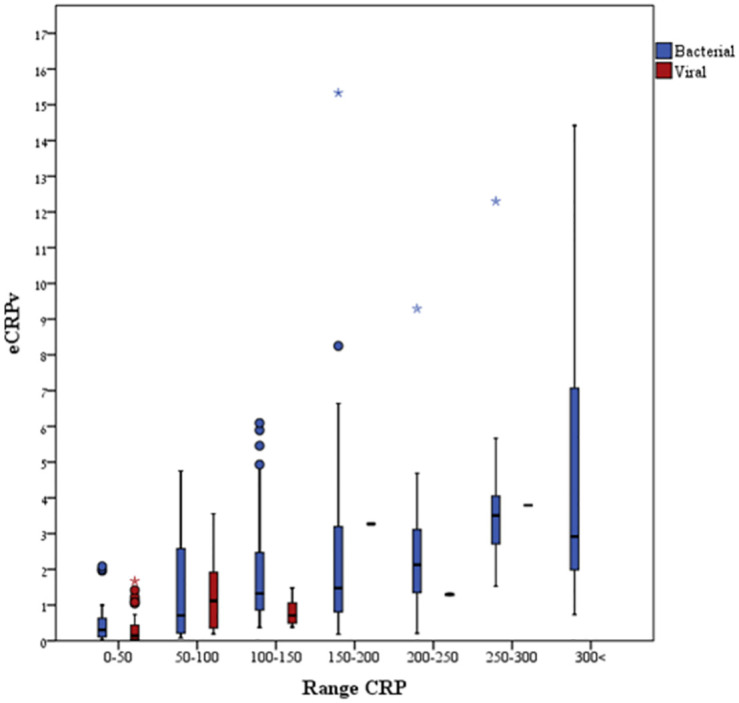
Results: Bacterial patients presented with higher CRP levels (133 mg/L) upon admission compared to viral patients (23.31 mg/L) (P < 0.001). Their median value of eCRPv velocity was 4 times higher compared to the viral patients (1.1 mg/L/h compared 0.25 mg/L/h, P < 0.001). Moreover, in intermediate values of CRP (100-150 mg/L) upon admission, in which the differential diagnosis is controversial, high eCRPv is indicative of bacterial infection, eCRPv >4 mg/L/h represents only bacterial patients.
Conclusions: During an acute febrile illness, the eCRPv value can be used for rapid differentiation between bacterial and viral infection, especially in patients with high CRP values. This capability can potentially expedite the provision of appropriate therapeutic management. Further research and validation may open new applications of the kinetics of inflammation for rapid diagnosis of an infectious vs. a viral source of fever.
Copyright: © 2022 Largman-Chalamish et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Craig JC, Williams GJ, Jones M, Codarini M, Macaskill P, Hayen A, et al.. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: Prospective cohort study of 15 781 febrile illnesses. BMJ. 2010;340(7754):1015. doi: 10.1136/bmj.c1594 - DOI - PMC - PubMed
-
- Furman D, Campisi J, Verdin E, Carrera-Bastos P, Targ S, Franceschi C, et al.. Chronic inflammation in the etiology of disease across the life span. Nat Med [Internet]. 2019;25(12):1822–32. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31806905 - PMC - PubMed
-
- World Health Organization. C-reactive protein concentrations as a marker of inflammation or infection for interpreting biomarkers of micronutrient status. Who/Nmh/Nhd/Epg/147. 2014; Accessed at 15.12.2018.
-
- Chan YL, Liao HC, Tsay PK, Chang SS, Chen JC, Liaw SJ. C-reactive protein as an indicator of bacterial infection of adult patients in the emergency department. Chang Gung Med J. 2002;25(7):437–45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
