

Acute ischaemic stroke: recent advances in reperfusion treatment
- PMID: 36477996
- PMCID: PMC10079392
- DOI: 10.1093/eurheartj/ehac684
Acute ischaemic stroke: recent advances in reperfusion treatment
Abstract
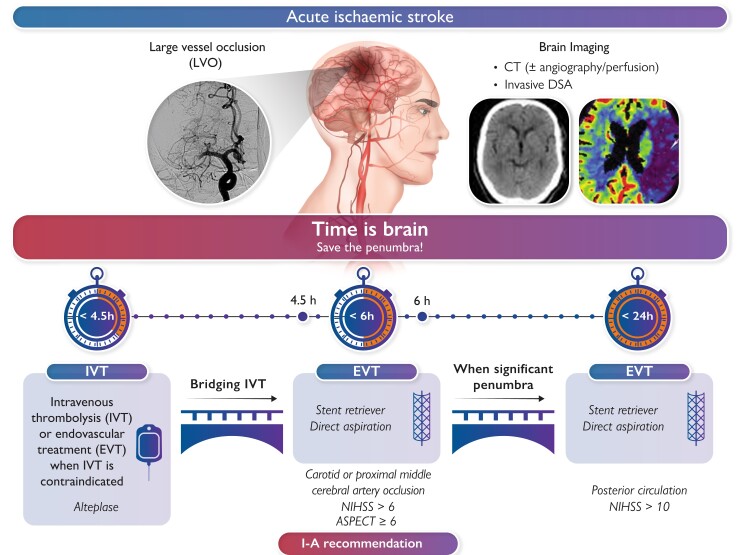
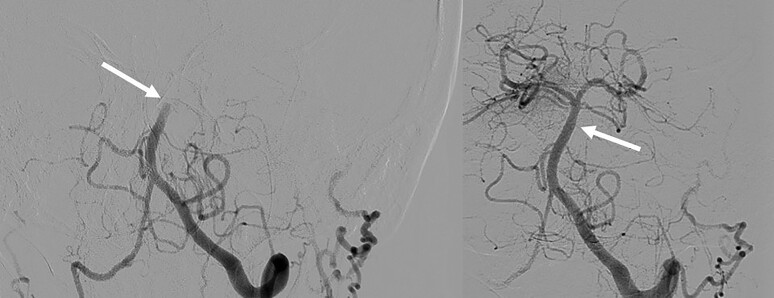
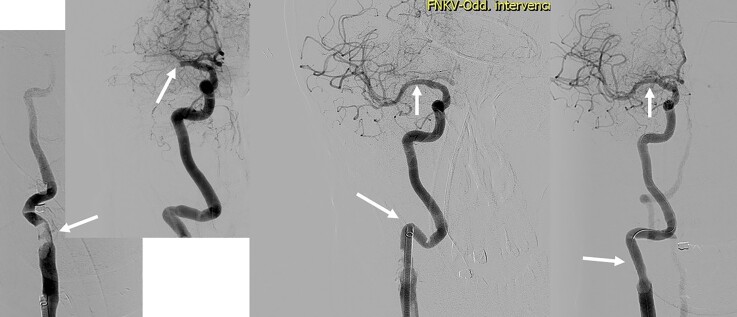
During the last 5-7 years, tremendous progress was achieved in the reperfusion treatment of acute ischaemic stroke during its first few hours from symptom onset. This review summarizes the latest evidence from randomized clinical trials and prospective registries with a focus on endovascular treatment using stent retrievers, aspiration catheters, thrombolytics, and (in selected patients) carotid stenting. Novel approaches in prehospital (mobile interventional stroke teams) and early hospital (direct transfer to angiography) management are described, and future perspectives ('all-in-one' laboratories with angiography and computed tomography integrated) are discussed. There is reasonable chance for patients with moderate-to-severe acute ischaemic stroke to survive without permanent sequelae when the large-vessel occlusion is removed by means of modern pharmaco-mechanic approach. Catheter thrombectomy is now the golden standard of acute stroke treatment. The role of cardiologists in stroke is expanding from diagnostic help (to reveal the cause of stroke) to acute therapy in those regions where such up-to-date Class I. A treatment is not yet available.
Keywords: Acute stroke; Endovascular; Thrombectomy; Thrombolysis.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest All authors declare no conflict of interest for this contribution.
Figures
Comment in
-
Focus issue on vascular biology and medicine spanning from management of stroke to new therapeutic targets in aortic dissection and pulmonary hypertension.Eur Heart J. 2023 Apr 7;44(14):1193-1196. doi: 10.1093/eurheartj/ehad198. Eur Heart J. 2023. PMID: 37024112 No abstract available.
References
-
- Wagner A, Schebesch KM, Isenmann S, Steinbrecher A, Kapapa T, Zeman F, et al. Interdisciplinary decision making in hemorrhagic stroke based on CT imaging—differences between neurologists and neurosurgeons regarding estimation of patients’ symptoms, Glasgow Coma Scale, and National Institutes of Health Stroke Scale. Front Neurol 2019;10:997. 10.3389/fneur.2019.00997 - DOI - PMC - PubMed
-
- Lip GYH, Lane DA, Lenarczyk R, Boriani G, Doehner W, Benjamin LA, et al. Integrated care for optimizing the management of stroke and associated heart disease: a position paper of the European Society of Cardiology Council on Stroke. Eur Heart J 2022;43:2442–2460. 10.1093/eurheartj/ehac245 - DOI - PMC - PubMed
-
- Nardai S, Lanzer P, Abelson M, Baumbach A, Doehner W, Hopkins LN, et al. Interdisciplinary management of acute ischaemic stroke: current evidence training requirements for endovascular stroke treatment: position paper from the ESC Council on Stroke and the European Association for Percutaneous Cardiovascular Interventions with the support of the European Board of Neurointervention. Eur Heart J 2021;42:298–307. 10.1093/eurheartj/ehaa833 - DOI - PubMed
