

Treatment times, functional outcome, and hemorrhage rates after switching to tenecteplase for stroke thrombolysis: Insights from the TETRIS registry
- PMID: 36478758
- PMCID: PMC9720850
- DOI: 10.1177/23969873221113729
Treatment times, functional outcome, and hemorrhage rates after switching to tenecteplase for stroke thrombolysis: Insights from the TETRIS registry
Abstract
Introduction: The encouraging efficacy and safety data on intravenous thrombolysis with tenecteplase in ischemic stroke and its practical advantages motivated our centers to switch from alteplase to tenecteplase. We report its impact on treatment times and clinical outcomes.
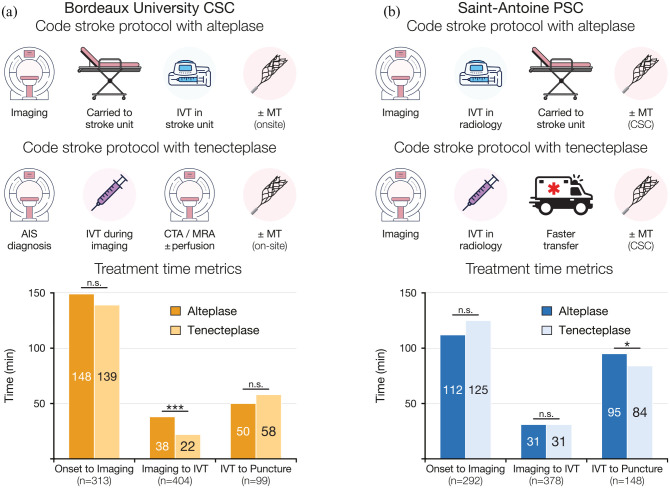
Methods: We retrospectively analyzed clinical and procedural data of patients treated with alteplase or tenecteplase in a comprehensive (CSC) and a primary stroke center (PSC), which transitioned respectively in 2019 and 2018. Tenecteplase enabled in-imaging thrombolysis in the CSC. The main outcomes were the imaging-to-thrombolysis and thrombolysis-to-puncture times. We assessed the association of tenecteplase with 3-month functional independence and parenchymal hemorrhage (PH) with multivariable logistic models.
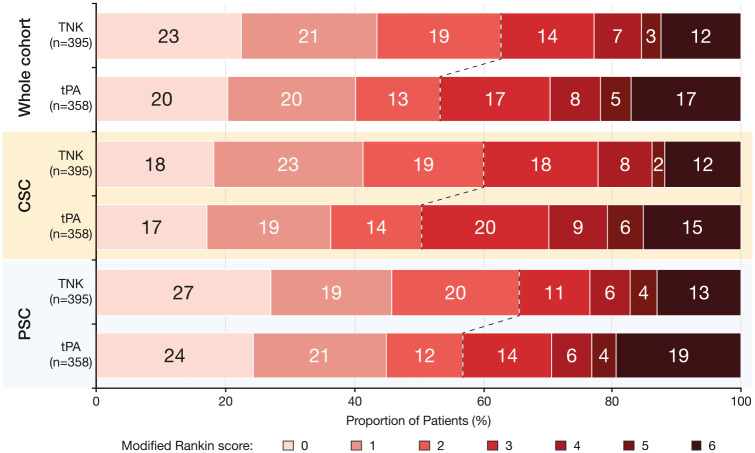
Results: We included 795 patients, 387 (48.7%) received alteplase and 408 (51.3%) tenecteplase. Both groups (tenecteplase vs alteplase) were similar in terms of age (75 vs 76 years), baseline NIHSS score (7 vs 7.5) and proportion of patients treated with mechanical thrombectomy (24.1% vs 27.5%). Tenecteplase patients had shorter imaging-to-thrombolysis times (27 vs 36 min, p < 0.0001) mainly driven by patients treated in the CSC (22 vs 38 min, p < 0.001). In the PSC, tenecteplase patients had shorter thrombolysis-to-puncture times (84 vs 95 min, p = 0.02), reflecting faster interhospital transfer for MT. 3-month functional independence rate was higher in the tenecteplase group (62.8% vs 53.4%, p < 0.01). In the multivariable analysis, tenecteplase was significantly associated with functional independence (ORa 1.68, 95% CI 1.15-2.48, p < 0.01), but not with PH (ORa 0.68, 95% CI 0.41-1.12, p = 0.13).
Conclusion: Switch from alteplase to tenecteplase reduced process times and may improve functional outcome, with similar safety profile.
Keywords: Ischemic stroke; acute stroke therapy; process times; tenecteplase; thrombolysis.
© European Stroke Organisation 2022.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All reported disclosures were outside the submitted work. Dr. Laborne reports personal fees from Boehringer Ingelheim. Dr. Marnat reports personal fees from Stryker, Medtronic and Microvention. Prof. Clarençon reports personal fees from Medtronic, Guerbet, Balt Extrusion and Penumbra. Dr. Chausson reports a grant and personal fees from Boehringer Ingelheim and Bristol Myers Squibb. Prof. Sibon reports personal fees from Astra-Zeneca, Bayer, BMS-Pfizer, Boehringer Ingelheim, Elsevier, Novonordisk, Servier and Medtronic. Prof. Alamowitch reports personal fees from the Astra-Zeneca, Bayer, BMS-Pfizer and Elsevier. No other disclosures were reported.
Figures

References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 Guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019; 50: e344–e418. - PubMed
-
- Campbell BCV, Mitchell PJ, Churilov L, et al. Tenecteplase versus alteplase before thrombectomy for ischemic stroke. New Engl J Medicine 2018; 378: 1573–1582. - PubMed
-
- Zhong CS, Beharry J, Salazar D, et al. Routine use of tenecteplase for thrombolysis in acute ischemic stroke. Stroke 2021; 52: 1087–1090. - PubMed
LinkOut - more resources
Full Text Sources
