

Effect of constraint-induced movement therapy on lower extremity motor dysfunction in post-stroke patients: A systematic review and meta-analysis
- PMID: 36479056
- PMCID: PMC9720264
- DOI: 10.3389/fneur.2022.1028206
Effect of constraint-induced movement therapy on lower extremity motor dysfunction in post-stroke patients: A systematic review and meta-analysis
Abstract
Objective: Constraint-induced movement therapy (CIMT) is a common treatment for upper extremity motor dysfunction after a stroke. However, whether it can effectively improve lower extremity motor function in stroke patients remains controversial. This systematic review comprehensively studies the current evidence and evaluates the effectiveness of CIMT in the treatment of post-stroke lower extremity motor dysfunction.
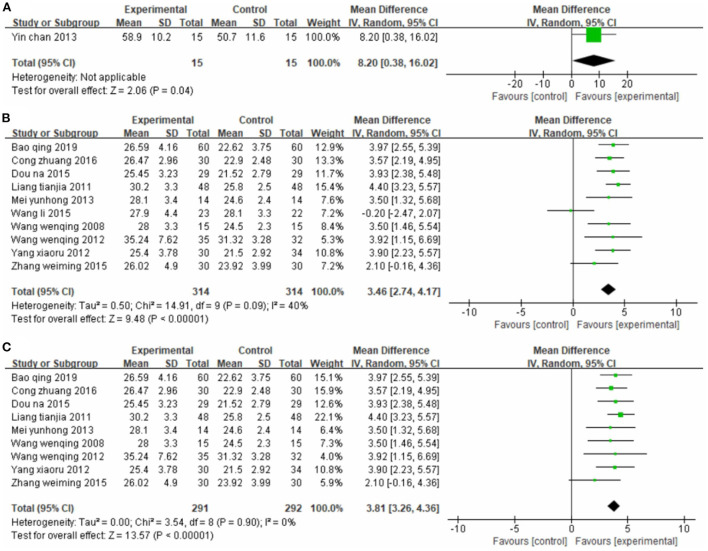
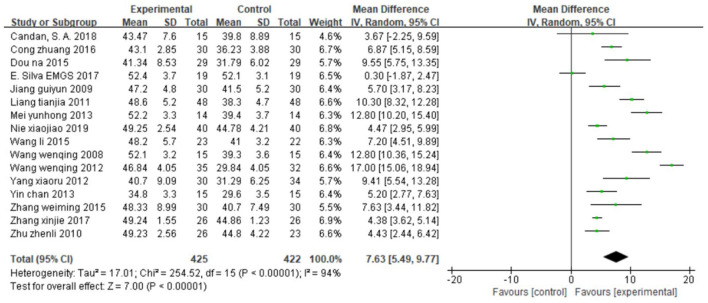
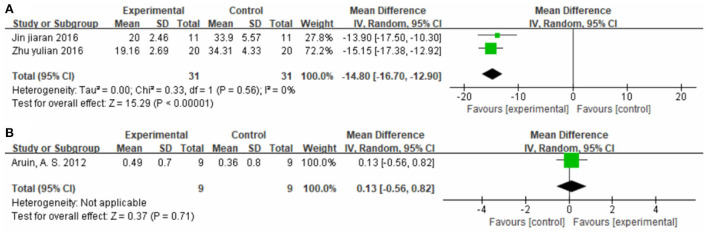
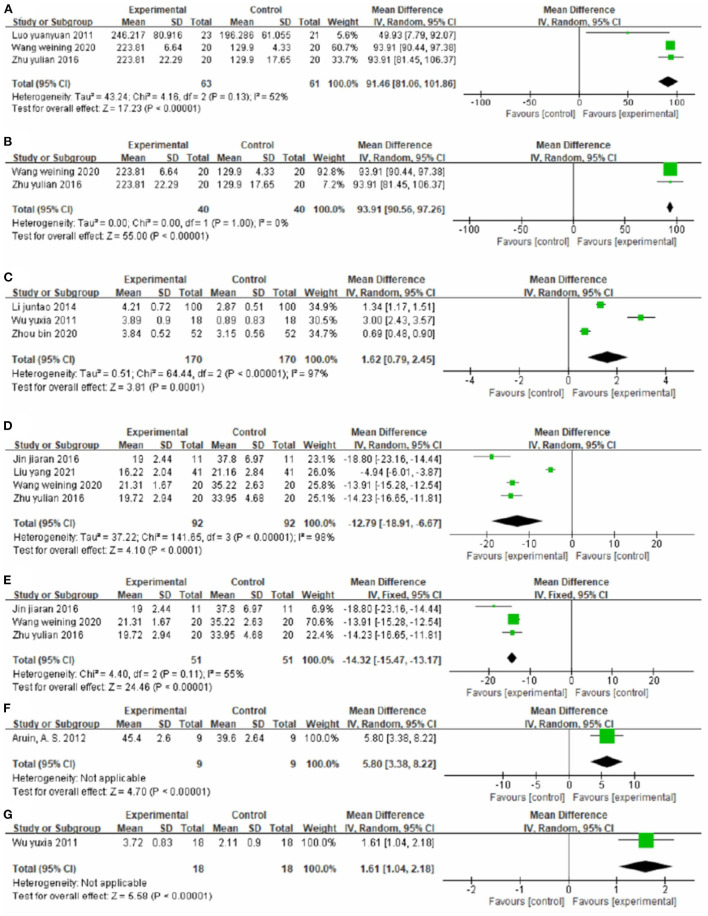
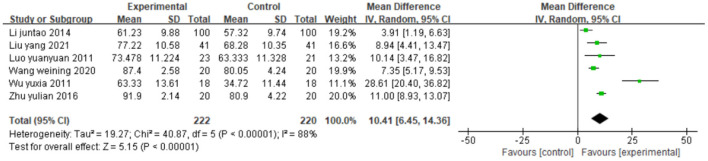
Methods: We comprehensively searched randomized controlled trials related to this study in eight electronic databases (PubMed, Embase, The Cochrane Library, Web of Science, CBM, CNKI, WAN FANG, and VIP). We evaluated CIMT effectiveness against post-stroke lower extremity motor dysfunction based on the mean difference and corresponding 95% confidence interval (95% CI). We assessed methodological quality based on the Cochrane Bias Risk Assessment Tool. After extracting the general information, mean, and standard deviation of the included studies, we conducted a meta-analysis using RevMan 5.3 and Stata 16.0. The primary indicator was the Fugl-Meyer Assessment scale on lower limbs (FMA-L). The secondary indicators were the Berg balance scale (BBS), 10-meter walk test (10MWT), gait speed (GS), 6-min walk test (6MWT), functional ambulation category scale (FAC), timed up and go test (TUGT), Brunnstrom stage of lower limb function, weight-bearing, modified Barthel index (MBI), functional independence measure (FIM), stroke-specific quality of life questionnaire (SSQOL), World Health Organization quality of life assessment (WHOQOL), and National Institute of Health stroke scale (NIHSS).
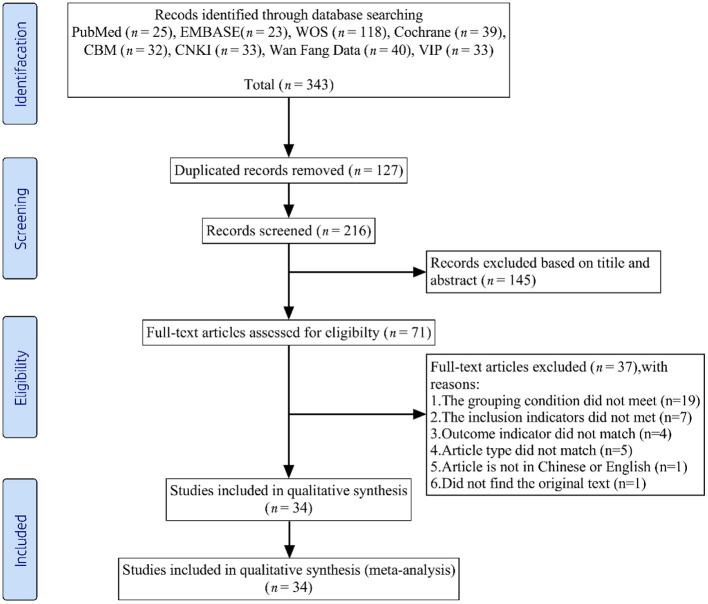
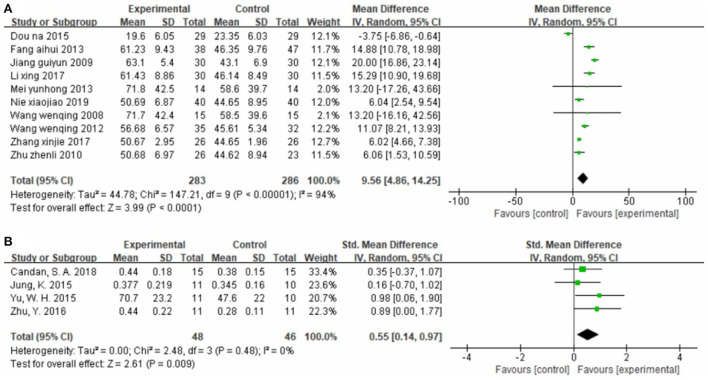
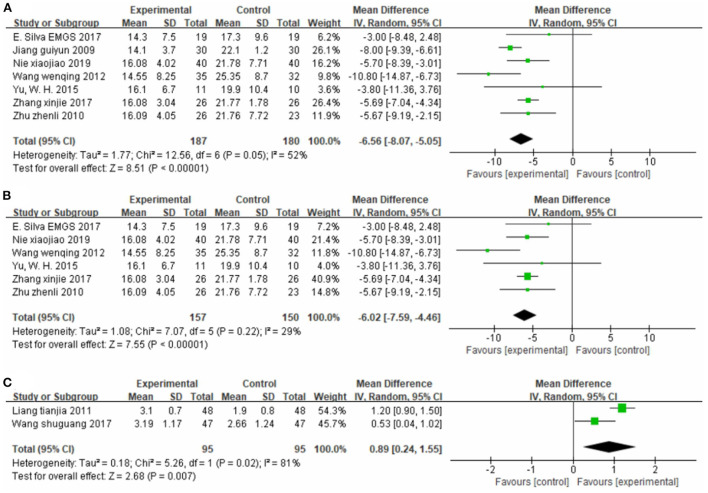
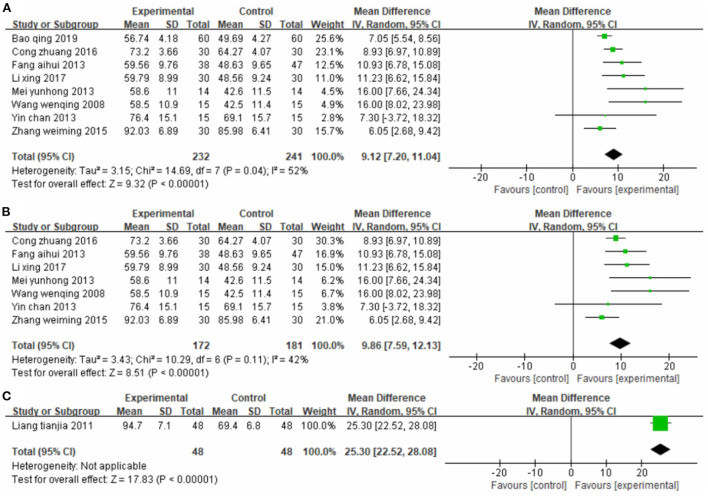
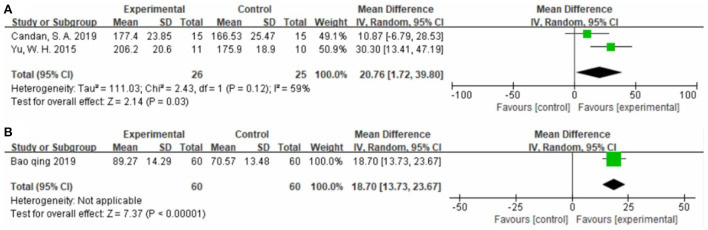
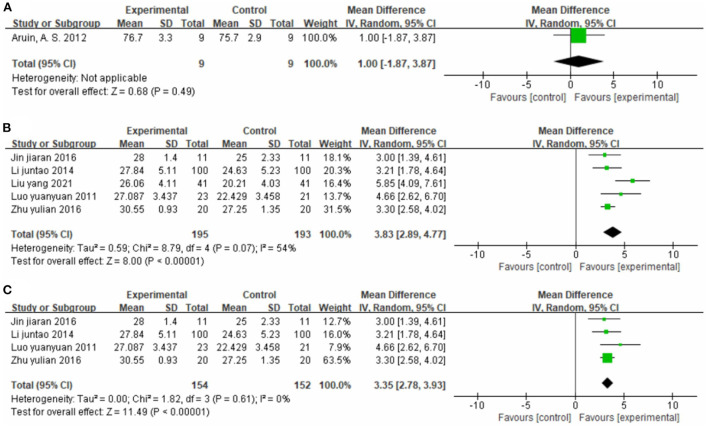
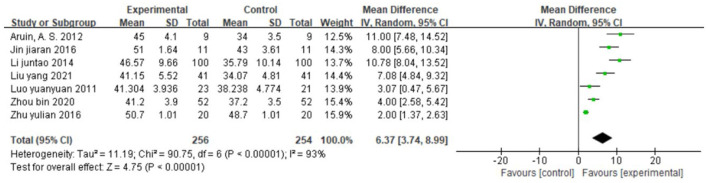
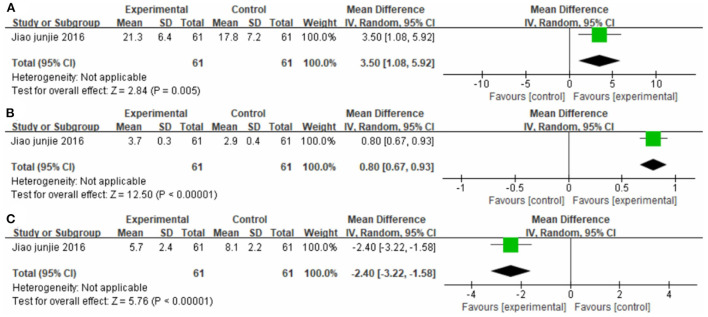
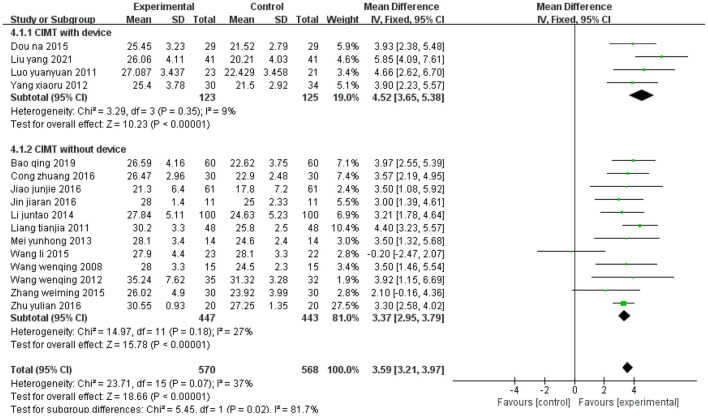
Results: We initially identified 343 relevant studies. Among them, 34 (totaling 2,008 patients) met the inclusion criteria. We found that patients treated with CIMT had significantly better primary indicator (FMA-L) scores than those not treated with CIMT. The mean differences were 3.46 (95% CI 2.74-4.17, P < 0.01, I2 = 40%) between CIMT-treated and conventional physiotherapy-treated patients, 3.83 (95% CI 2.89-4.77, P < 0.01, I2 = 54%) between patients treated with CIMT plus conventional physiotherapy and patients treated only with conventional physiotherapy, and 3.50 (95% CI 1.08-5.92, P < 0.01) between patients treated with CIMT plus western medicine therapy and those treated only with western medicine therapy. The secondary indicators followed the same trend. The subgroup analysis showed that lower extremity CIMT with device seemed to yield a higher mean difference in FMA-L scores than lower extremity CIMT without device (4.52, 95% CI = 3.65-5.38, P < 0.01 and 3.37, 95% CI = 2.95-3.79, P < 0.01, respectively).
Conclusion: CIMT effectively improves lower extremity motor dysfunction in post-stroke patients; however, the eligible studies were highly heterogeneous.Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=277466.
Keywords: constraint-induced movement therapy; lower extremity; meta-analysis; motor dysfunction; post-stroke.
Copyright © 2022 Zhou, Tu, Cui, Gao, Yi, Wang, Hao, Li and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Does whole-body vibration training have a positive effect on balance and walking function in patients with stroke? A meta-analysis.Front Hum Neurosci. 2023 Jan 4;16:1076665. doi: 10.3389/fnhum.2022.1076665. eCollection 2022. Front Hum Neurosci. 2023. PMID: 36684839 Free PMC article.
-
Constraint-induced movement therapy for rehabilitation of arm dysfunction after stroke in adults: an evidence-based analysis.Ont Health Technol Assess Ser. 2011;11(6):1-58. Epub 2011 Nov 1. Ont Health Technol Assess Ser. 2011. PMID: 23074418 Free PMC article.
-
Efficacy and safety of moxibustion treatment for upper extremity pain disorder and motor impairment in patients with stage I post-stroke shoulder-hand syndrome: a systematic review and meta-analysis of randomized controlled trials.Front Neurol. 2025 May 23;16:1530069. doi: 10.3389/fneur.2025.1530069. eCollection 2025. Front Neurol. 2025. PMID: 40488201 Free PMC article.
-
The effect and safety of constraint-induced movement therapy for post-stroke motor dysfunction: a meta-analysis and trial sequential analysis.Front Neurol. 2023 Apr 18;14:1137320. doi: 10.3389/fneur.2023.1137320. eCollection 2023. Front Neurol. 2023. PMID: 37144004 Free PMC article.
-
Lower-extremity constraint-induced movement therapy improved motor function, mobility, and walking after stroke.Eur J Phys Rehabil Med. 2023 Apr;59(2):136-144. doi: 10.23736/S1973-9087.23.07683-9. Epub 2023 Mar 9. Eur J Phys Rehabil Med. 2023. PMID: 36892520 Free PMC article.
Cited by
-
Post-stroke health-related quality of life following lower-extremity constraint-induced movement therapy - An observational survey study.PLoS One. 2025 May 8;20(5):e0323290. doi: 10.1371/journal.pone.0323290. eCollection 2025. PLoS One. 2025. PMID: 40341838 Free PMC article.
References
-
- Preetha K, Vimala U, Kamalakannan M. A study to compare task-based mirror therapy versus constraint induced movement therapy for hand function in hemiplegic subjects. Biomedicine (india). (2021) 41:665-668. 10.51248/.v41i3.1204 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous