

Biological and clinical review of IORT-induced wound fluid in breast cancer patients
- PMID: 36479071
- PMCID: PMC9720171
- DOI: 10.3389/fonc.2022.980513
Biological and clinical review of IORT-induced wound fluid in breast cancer patients
Abstract
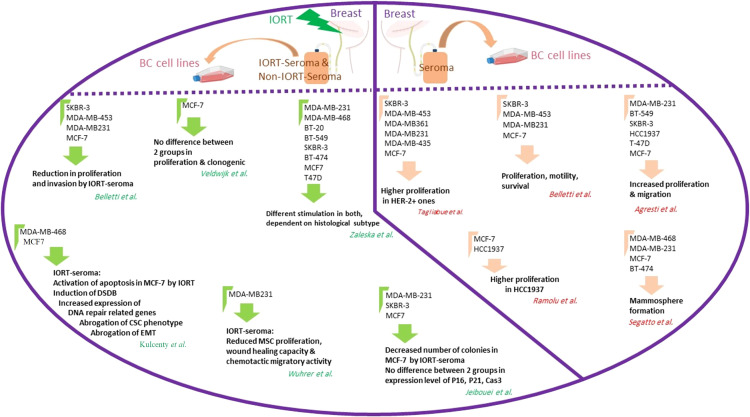
Intraoperative radiotherapy (IORT) has become a growing therapy for early-stage breast cancer (BC). Some studies claim that wound fluid (seroma), a common consequence of surgical excision in the tumor cavity, can reflect the effects of IORT on cancer inhibition. However, further research by our team and other researchers, such as analysis of seroma composition, affected cell lines, and primary tissues in two-dimensional (2D) and three-dimensional (3D) culture systems, clarified that seroma could not address the questions about IORT effectiveness in the surgical site. In this review, we mention the factors involved in tumor recurrence, direct or indirect effects of IORT on BC, and all the studies associated with BC seroma to attain more information about the impact of IORT-induced seroma to make a better decision to remove or remain after surgery and IORT. Finally, we suggest that seroma studies cannot decipher the mechanisms underlying the effectiveness of IORT in BC patients. The question of whether IORT-seroma has a beneficial effect can only be answered in a trial with a clinical endpoint, which is not even ongoing.
Keywords: IORT; breast cancer; personalized medicine; seroma; tumor microenvironment.
Copyright © 2022 Jeibouei, Shams, Mohebichamkhorami, Sanooghi, Faal, Akbari and Zali.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Comparison of seroma production in breast conserving surgery with or without intraoperative radiotherapy as tumour bed boost.Arch Gynecol Obstet. 2016 Oct;294(4):861-6. doi: 10.1007/s00404-016-4124-8. Epub 2016 Jun 2. Arch Gynecol Obstet. 2016. PMID: 27256339
-
Risk factors for seroma evacuation in breast cancer patients treated with intraoperative radiotherapy.Rep Pract Oncol Radiother. 2016 May-Jun;21(3):225-31. doi: 10.1016/j.rpor.2016.03.003. Epub 2016 Mar 29. Rep Pract Oncol Radiother. 2016. PMID: 27601955 Free PMC article.
-
Postoperative seroma formation after intraoperative radiotherapy using low-kilovoltage X-rays given during breast-conserving surgery.Int J Radiat Oncol Biol Phys. 2010 Jul 15;77(4):1140-5. doi: 10.1016/j.ijrobp.2009.06.008. Epub 2009 Oct 14. Int J Radiat Oncol Biol Phys. 2010. PMID: 19836152
-
Intraoperative radiotherapy in breast cancer: Alterations to the tumor microenvironment and subsequent biological outcomes (Review).Mol Med Rep. 2023 Dec;28(6):231. doi: 10.3892/mmr.2023.13118. Epub 2023 Oct 27. Mol Med Rep. 2023. PMID: 37888611 Free PMC article. Review.
-
Intraoperative radiotherapy (IORT) as boost in breast cancer.Radiat Oncol. 2017 Jan 19;12(1):23. doi: 10.1186/s13014-016-0749-9. Radiat Oncol. 2017. PMID: 28103903 Free PMC article. Review.
References
-
- Fitzmaurice C, Abate D, Abbasi N. Global burden of disease cancer collaboration. global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990to 2017: A systemic analysis for the global burden of disease study (vol 5, pg 1749, 2019). JAMA Oncol (2020) 6(3):444–4. doi: 10.1001/jamaoncol.2019.2996 - DOI - PMC - PubMed
-
- Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. . Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. New Engl J Med (2002) 347(16):1233–41. doi: 10.1056/NEJMoa022152 - DOI - PubMed
-
- Vaidya JS, Bulsara M, Baum M, Wenz F, Massarut S, Pigorsch S, et al. . Long term survival and local control outcomes from single dose targeted intraoperative radiotherapy during lumpectomy (TARGIT-IORT) for early breast cancer: TARGIT-a randomised clinical trial. Bmj (2020) 370:m2836. doi: 10.1136/bmj.m2836 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources