

Effects of Linagliptin and Pioglitazone on Fracture Healing in an Experimental Type 2 Diabetes Rat Model
- PMID: 36479259
- PMCID: PMC9721100
- DOI: 10.7759/cureus.32204
Effects of Linagliptin and Pioglitazone on Fracture Healing in an Experimental Type 2 Diabetes Rat Model
Abstract
Aim: Our study aimed to examine the effects of Linagliptin, Pioglitazone, and their combination on fracture healing in a diabetes rat femur fracture model.
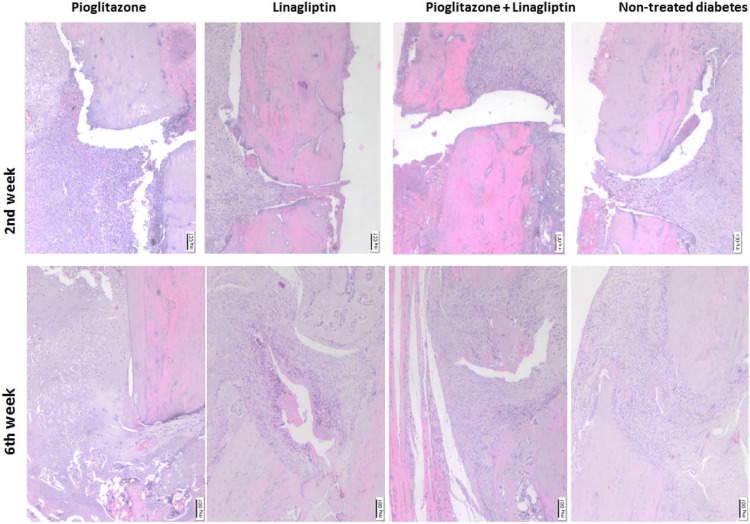
Material and methods: Type 2 diabetes mellitus (T2DM) induced rats were randomly divided into four groups: non-treated diabetes group (TD), Pioglitazone group (P), Linagliptin group (L), and Pioglitazone and Linagliptin group (PL). Daily oral dosage of pioglitazone (10 mg/kg/day), linagliptin (10 mg/kg/day), and their combination were administered. Femur fractures were stabilized intramedullary. At weeks 2 and 6, rats were sacrificed for evaluation radiologically, biomechanically, histopathologically, histomorphometrically, and immunohistochemically.
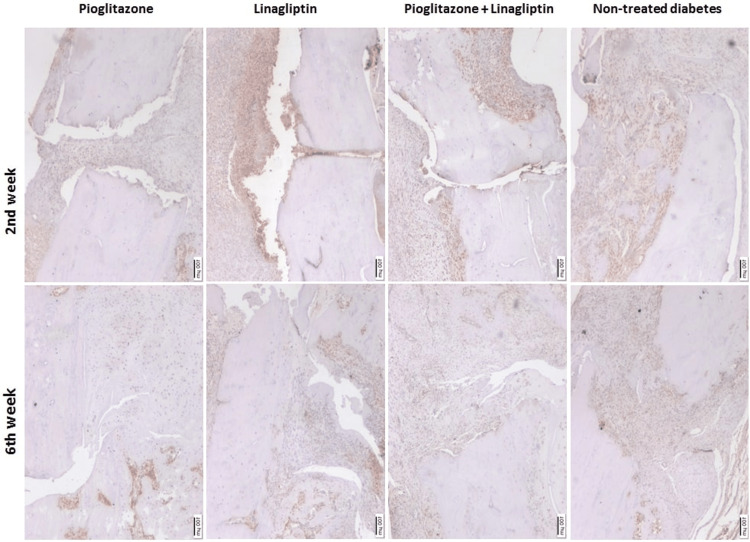
Results: Flexural strength of the L and PL groups were significantly higher compared to the P group. The highest healing score was in the L group and lowest in the P group, while the highest inflammation score was in the P group and lowest in the L group. A cluster of differentiation (CD) CD 34 reactivity was highest in the L group and lowest in the PL group.
Conclusion: Linagliptin treatment significantly increased histological healing scores, callus volume, biomechanical strength, and vascularity, however, minimized the inflammatory process, which was increased by pioglitazone. The combination of linagliptin and pioglitazone restored BMD and increased biomechanical strength. Linagliptin monotherapy is rarely indicated; hence, T2DM patients with a high risk of bone fractures can be considered for combined therapy of pioglitazone and linagliptin.
Keywords: bone healing; linagliptin; pioglitazone; streptozotocin; type 2 diabetes.
Copyright © 2022, Mraja et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures








Similar articles
-
Efficacy and safety of initial combination therapy with linagliptin and pioglitazone in patients with inadequately controlled type 2 diabetes: a randomized, double-blind, placebo-controlled study.Diabetes Obes Metab. 2011 Jul;13(7):653-61. doi: 10.1111/j.1463-1326.2011.01391.x. Diabetes Obes Metab. 2011. PMID: 21410628 Clinical Trial.
-
The effects of cephalexin on fracture healing in a rat femur fracture model.Jt Dis Relat Surg. 2023 Apr 26;34(2):413-424. doi: 10.52312/jdrs.2023.994. Jt Dis Relat Surg. 2023. PMID: 37462646 Free PMC article.
-
The effect of different irrigation solutions on fracture healing in a rat femur fracture model.Jt Dis Relat Surg. 2021;32(1):144-151. doi: 10.5606/ehc.2021.77358. Epub 2021 Jan 6. Jt Dis Relat Surg. 2021. PMID: 33463430 Free PMC article.
-
Linagliptin: a review of its use in the management of type 2 diabetes mellitus.Drugs. 2012 Sep 10;72(13):1793-824. doi: 10.2165/11209570-000000000-00000. Drugs. 2012. PMID: 22913735 Review.
-
Comparison of dipeptidyl peptidase-4 inhibitors and pioglitazone combination therapy versus pioglitazone monotherapy in type 2 diabetes: A system review and meta-analysis.Medicine (Baltimore). 2018 Nov;97(46):e12633. doi: 10.1097/MD.0000000000012633. Medicine (Baltimore). 2018. PMID: 30431561 Free PMC article. Review.
References
-
- Bone mineral density and fracture risk in type-2 diabetes mellitus: the Rotterdam Study. de Liefde II, van der Klift M, de Laet CE, van Daele PL, Hofman A, Pols HA. Osteoporos Int. 2005;16:1713–1720. - PubMed
-
- Bone, sweet bone--osteoporotic fractures in diabetes mellitus. Hamann C, Kirschner S, Günther KP, Hofbauer LC. Nat Rev Endocrinol. 2012;8:297–305. - PubMed
-
- Bone metabolism in male patients with type 2 diabetes. Achemlal L, Tellal S, Rkiouak F, et al. Clin Rheumatol. 2005;24:493–496. - PubMed
-
- Osteoporosis-associated fracture and diabetes. Kurra S, Fink DA, Siris ES. Endocrinol Metab Clin North Am. 2014;43:233–243. - PubMed
-
- Bone quality assessment in type 2 diabetes mellitus. Dhaliwal R, Cibula D, Ghosh C, Weinstock RS, Moses AM. Osteoporos Int. 2014;25:1969–1973. - PubMed
LinkOut - more resources
Full Text Sources