

Patellar Resurfacing in Primary Total Knee Arthroplasty: A Meta-analysis and Trial Sequential Analysis of 50 Randomized Controlled Trials
- PMID: 36479594
- PMCID: PMC9891932
- DOI: 10.1111/os.13392
Patellar Resurfacing in Primary Total Knee Arthroplasty: A Meta-analysis and Trial Sequential Analysis of 50 Randomized Controlled Trials
Abstract
Objective: During total knee arthroplasty, femur and tibia parts are regularly replaced, while resurfacing the patellar or not is an ongoing discussion. To compare revision rate, anterior knee pain rate, patient-reported outcome measures, complication, radiographic, and clinical outcomes after patellar resurfacing versus non-resurfacing in total knee arthroplasty.
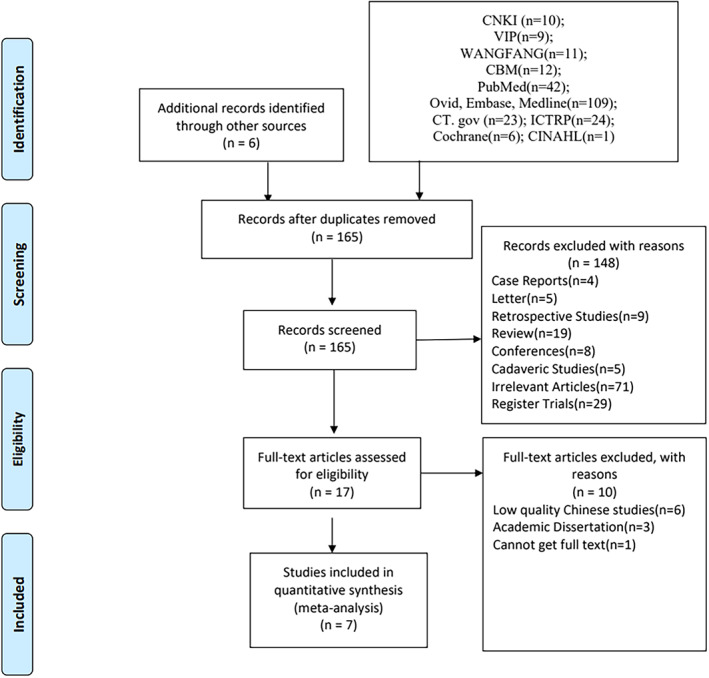
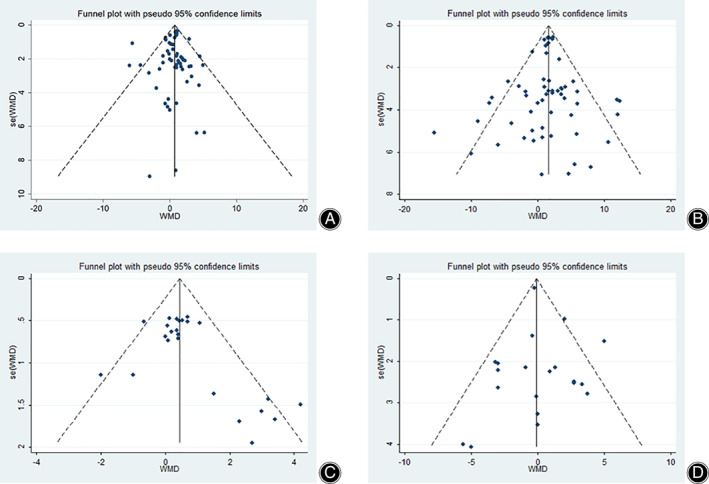
Methods: PubMed, Medline, EMBASE, CENTRAL, and CINAHL databases were searched on 25 April 2021 to enroll randomized controlled trials that compared patellar resurfacing versus non-resurfacing. We used the grading of recommendations assessment, development and evaluation (GRADE) framework to assess the certainty of evidence. Our primary outcome was revision rate and secondary outcomes was anterior knee pain rate. Outcomes were pooled using the random-effect model and presented as risk ratio (RR), or mean difference (MD), with 95% confidence interval (CI).
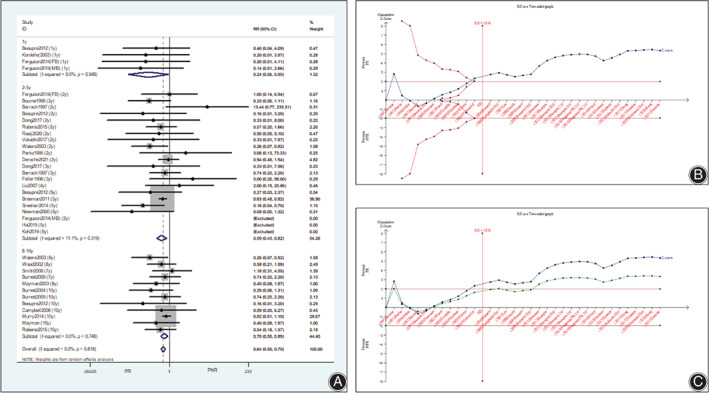
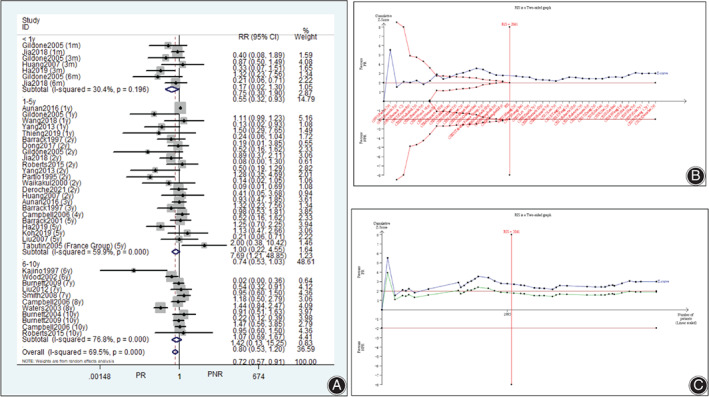
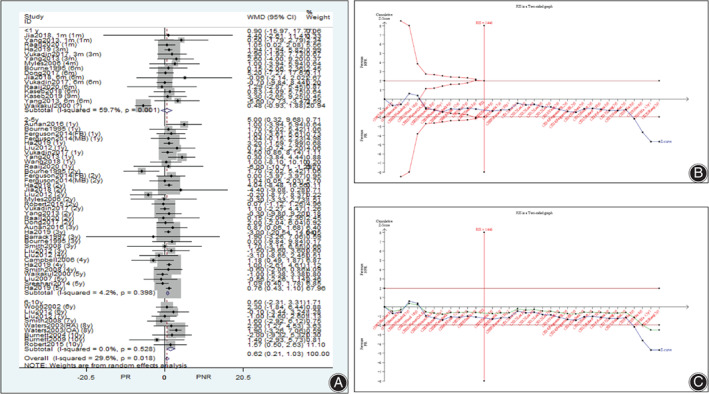
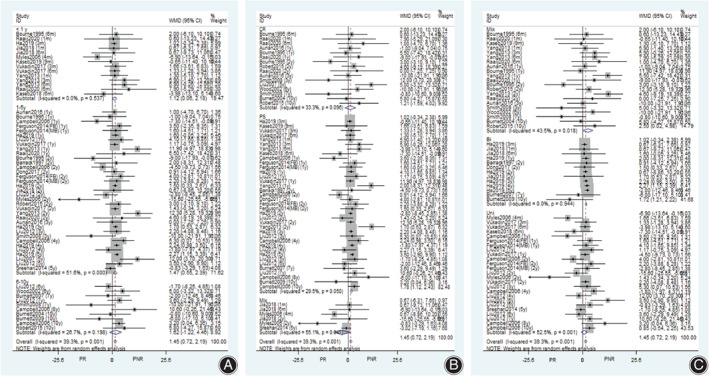
Results: Fifty studies (5586 knees) were included. Significant reductions in patellar revision rate (RR 0.41, 95% CI [0.19, 0.88]; P = 0.02; I2 = 24.20%) and non-patellar revision rate (RR 0.64, 95% CI [0.55, 0.75]; P < 0.001; I2 = 0%) were seen after patellar resurfacing. Patellar resurfacing significantly reduced the anterior knee pain rate than nonresurfacing (RR 0.72, 95% CI [0.57, 0.91]; P = 0.006; I2 = 69.5%). Significant differences in patient-reported outcome measures were found. However, these differences were inconsistent and lacked clinical importance. Patellar resurfacing resulted in a significant lower rate of patellar clunk (RR 0.58, 95% CI [0.38, 0.88]; P = 0.01; I2 = 0%), a higher patellar score (MD 1.24, 95% CI [0.67, 0.81]; P < 0.001; I2 = 73.8%), but prolonged surgical time (MD 8.59, 95% CI [5.27, 11.91]; P < 0.001; I2 = 88.8%).
Conclusions: The clear relationship is that patellar resurfacing reduces revisions, anterior knee pain, and patellar clunk. It will be interesting to compare the initial cost with the revision cost when required and cost-utility analysis with long-term results in future studies.
Keywords: Meta-analysis; Patellar resurfacing; Randomized controlled trials; Total knee arthroplasty.
© 2022 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Figures
Similar articles
-
Patellar resurfacing versus nonresurfacing in total knee arthroplasty: a meta-analysis of randomised controlled trials.Int Orthop. 2013 Jun;37(6):1075-83. doi: 10.1007/s00264-013-1866-9. Epub 2013 Mar 26. Int Orthop. 2013. PMID: 23529719 Free PMC article. Clinical Trial.
-
Patellar resurfacing versus retention in cruciate-retaining and posterior-stabilized total knee arthroplasty.Bone Joint J. 2023 Jun 1;105-B(6):622-634. doi: 10.1302/0301-620X.105B6.BJJ-2022-0970.R2. Bone Joint J. 2023. PMID: 37257851
-
Patellar Resurfacing in Primary Total Knee Arthroplasty: A Meta-Analysis of Randomized Controlled Trials.J Arthroplasty. 2019 Dec;34(12):3124-3132. doi: 10.1016/j.arth.2019.07.019. Epub 2019 Jul 20. J Arthroplasty. 2019. PMID: 31427130
-
Patellar resurfacing in primary total knee replacement: a meta-analysis.J Bone Joint Surg Am. 2012 Dec 19;94(24):2270-8. doi: 10.2106/JBJS.K.01257. J Bone Joint Surg Am. 2012. PMID: 23318618
-
Patellar resurfacing in total knee arthroplasty for osteoarthritis: a meta-analysis.Knee Surg Sports Traumatol Arthrosc. 2011 Sep;19(9):1460-6. doi: 10.1007/s00167-010-1365-0. Epub 2011 Jan 14. Knee Surg Sports Traumatol Arthrosc. 2011. PMID: 21234539 Review.
Cited by
-
Patellar resurfacing in contemporary total knee arthroplasty: Frequency of complications in a matched cohort.J Orthop. 2024 Sep 6;60:25-28. doi: 10.1016/j.jor.2024.09.006. eCollection 2025 Feb. J Orthop. 2024. PMID: 39345676
-
Functional outcome and cost effectiveness of patellar resurfacing and non-resurfacing in total knee arthroplasty: systematic review and meta-analysis.J Orthop Surg Res. 2025 May 20;20(1):492. doi: 10.1186/s13018-025-05892-z. J Orthop Surg Res. 2025. PMID: 40394607 Free PMC article.
-
SPECT/CT and triple-phase bone scan: A valuable diagnostic approach for identifying indications for secondary patellar resurfacing in patients with unexplained anterior knee pain post-TKA.Arthroplasty. 2025 Apr 2;7(1):15. doi: 10.1186/s42836-025-00300-7. Arthroplasty. 2025. PMID: 40170128 Free PMC article.
-
New evidence on patella resurfacing in modern total knee arthroplasty for all inflammatory arthritis in a mixed Asian population.J Clin Orthop Trauma. 2024 Oct 29;58:102798. doi: 10.1016/j.jcot.2024.102798. eCollection 2024 Nov. J Clin Orthop Trauma. 2024. PMID: 39564590
-
When to Do Selective Patellar Resurfacing in Total Knee Arthroplasty: A Decision-Making Algorithm Based on Pre-operative and Intra-operative Findings.Indian J Orthop. 2023 Dec 5;58(1):30-39. doi: 10.1007/s43465-023-01039-6. eCollection 2024 Jan. Indian J Orthop. 2023. PMID: 38161405 Free PMC article.
References
-
- Allen W, Eichinger J, Friedman R. Resurfaced versus non‐resurfaced patella in total knee arthroplasty. J Knee Surg. 2019;32(7):611–5. - PubMed
-
- NG157, N.g. , Joint replacement (primary): hip, knee and shoulder [L] Evidence review for patella resurfacing . Intervention evidence review underpinning recommendation 1.7.2 and the research recommendation in the NICE guideline, 2020.
-
- Teel AJ, Esposito JG, Lanting BA, Howard JL, Schemitsch EH. Patellar resurfacing in primary total knee arthroplasty: a meta‐analysis of randomized controlled trials. J Arthroplasty. 2019;34(12):3124–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
