

Development of Machine Learning Algorithms Incorporating Electronic Health Record Data, Patient-Reported Outcomes, or Both to Predict Mortality for Outpatients With Cancer
- PMID: 36480775
- PMCID: PMC10166444
- DOI: 10.1200/CCI.22.00073
Development of Machine Learning Algorithms Incorporating Electronic Health Record Data, Patient-Reported Outcomes, or Both to Predict Mortality for Outpatients With Cancer
Abstract
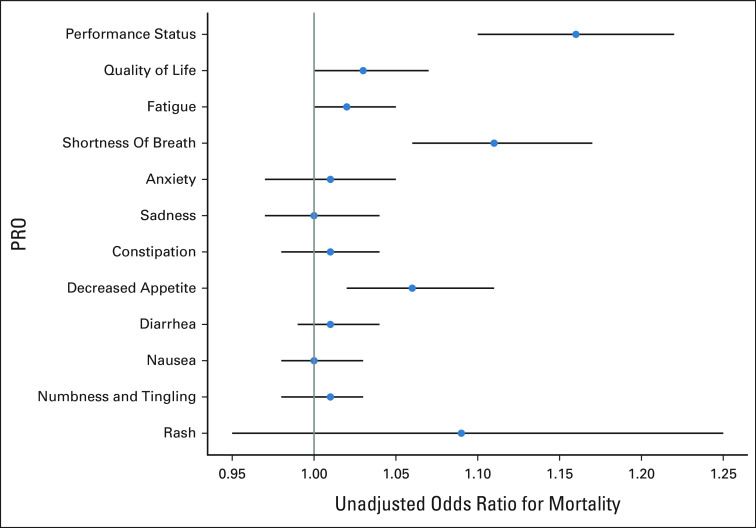
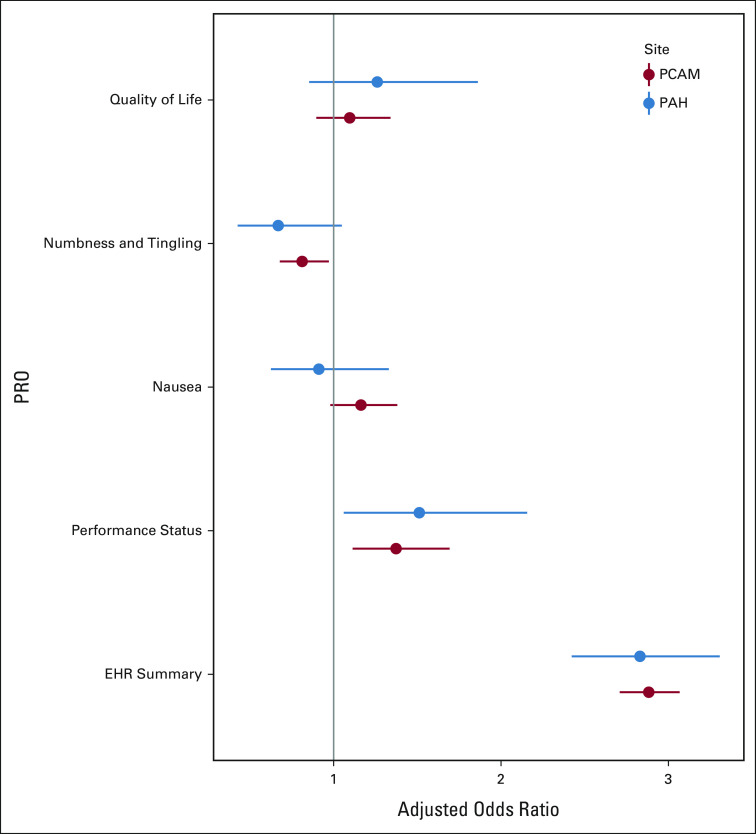
Purpose: Machine learning (ML) algorithms that incorporate routinely collected patient-reported outcomes (PROs) alongside electronic health record (EHR) variables may improve prediction of short-term mortality and facilitate earlier supportive and palliative care for patients with cancer.
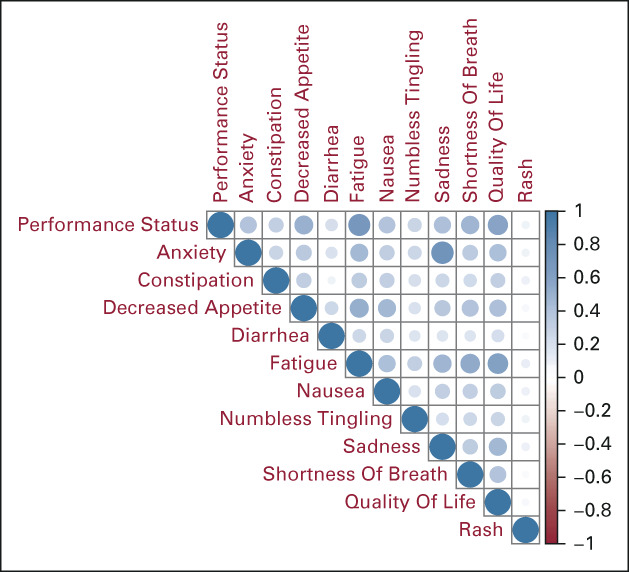
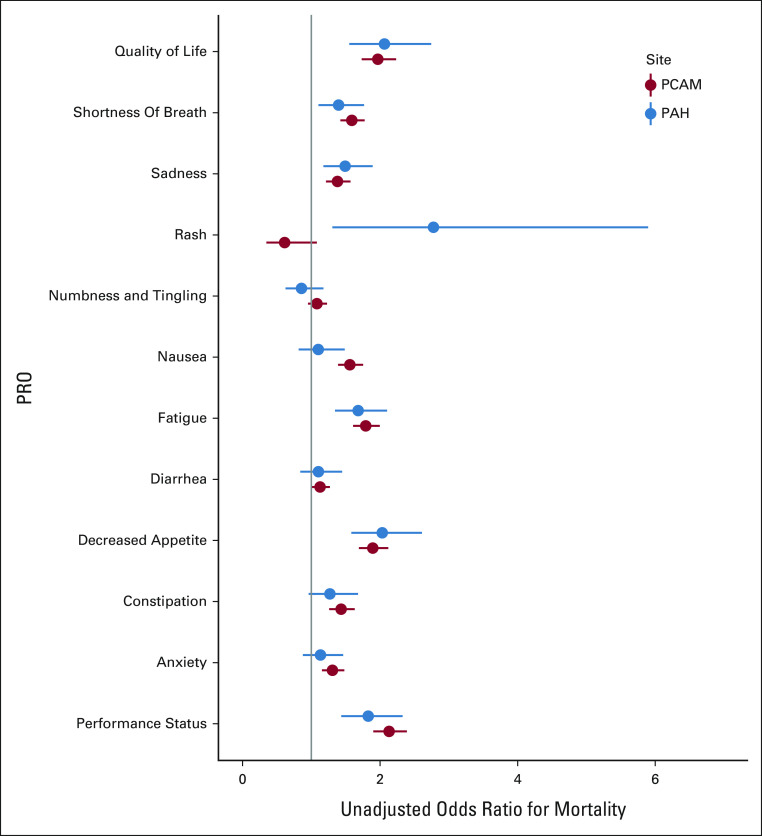
Methods: We trained and validated two-phase ML algorithms that incorporated standard PRO assessments alongside approximately 200 routinely collected EHR variables, among patients with medical oncology encounters at a tertiary academic oncology and a community oncology practice.
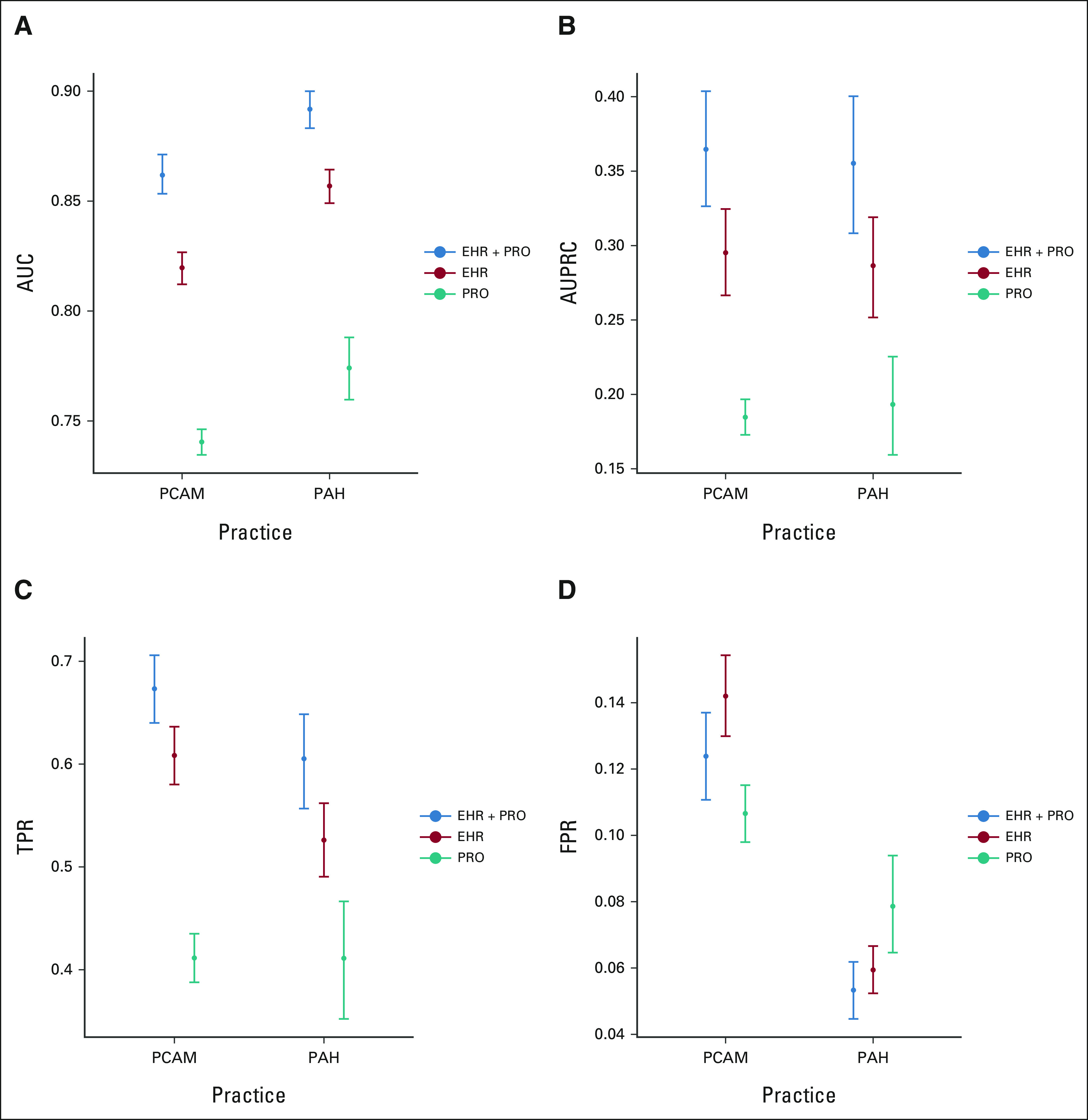
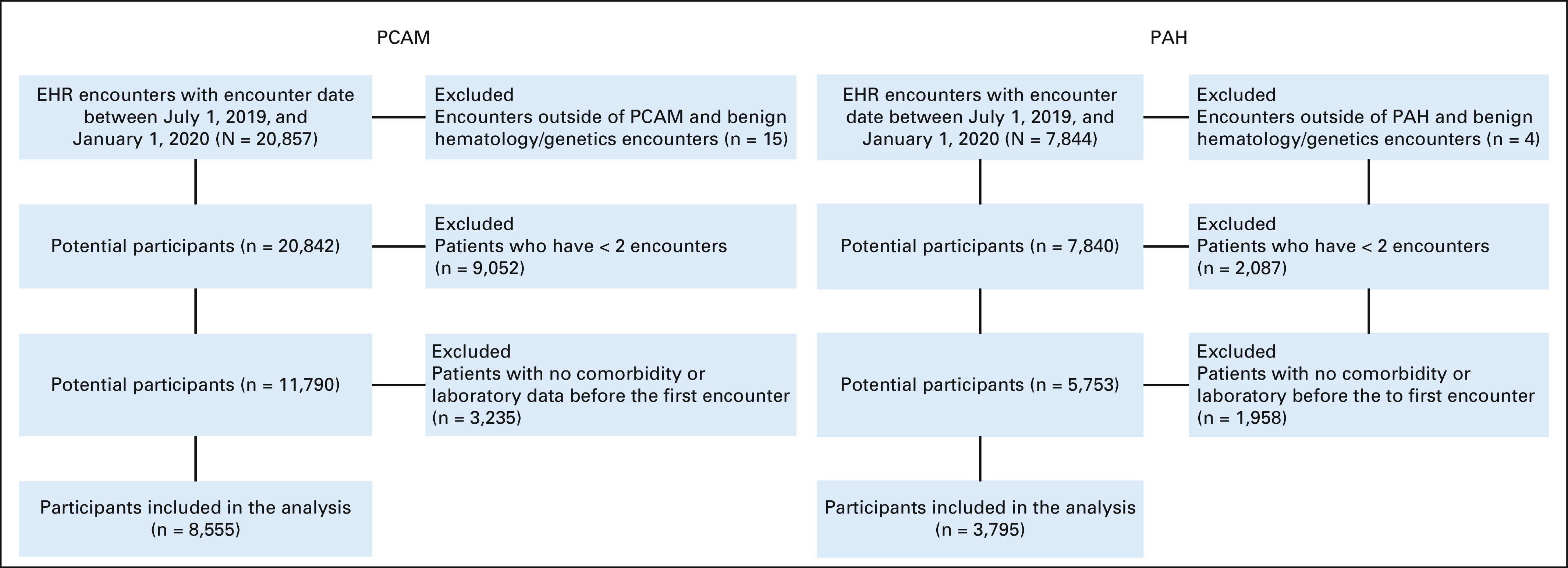
Results: Among 12,350 patients, 5,870 (47.5%) completed PRO assessments. Compared with EHR- and PRO-only algorithms, the EHR + PRO model improved predictive performance in both tertiary oncology (EHR + PRO v EHR v PRO: area under the curve [AUC] 0.86 [0.85-0.87] v 0.82 [0.81-0.83] v 0.74 [0.74-0.74]) and community oncology (area under the curve 0.89 [0.88-0.90] v 0.86 [0.85-0.88] v 0.77 [0.76-0.79]) practices.
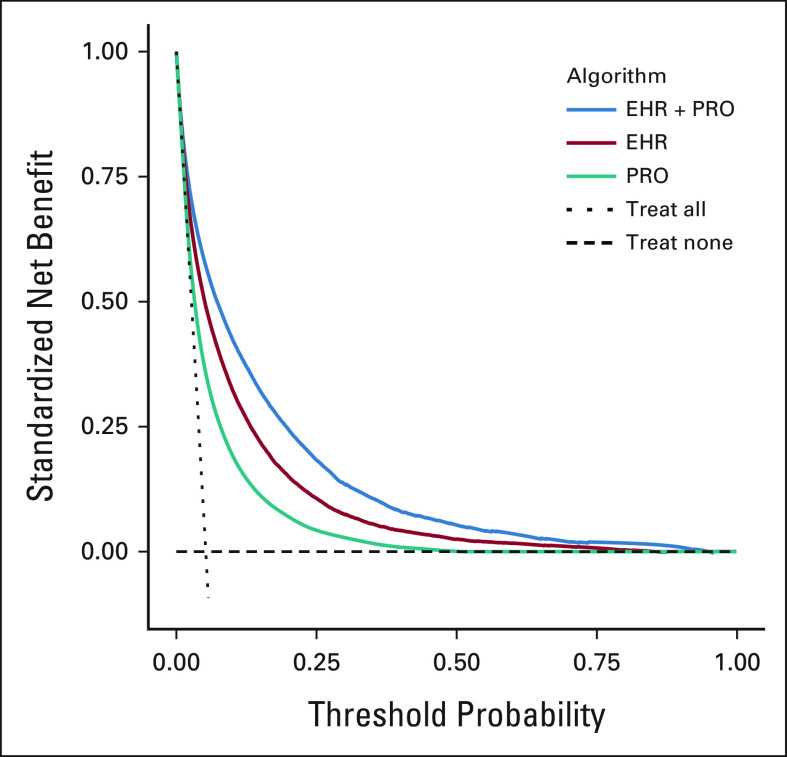
Conclusion: Routinely collected PROs contain added prognostic information not captured by an EHR-based ML mortality risk algorithm. Augmenting an EHR-based algorithm with PROs resulted in a more accurate and clinically relevant model, which can facilitate earlier and targeted supportive care for patients with cancer.
Conflict of interest statement
Figures
Similar articles
-
Use of Patient-Reported Outcomes in Risk Prediction Model Development to Support Cancer Care Delivery: A Scoping Review.JCO Clin Cancer Inform. 2024 Nov;8:e2400145. doi: 10.1200/CCI-24-00145. Epub 2024 Nov 1. JCO Clin Cancer Inform. 2024. PMID: 39486014 Free PMC article.
-
Validation of a Machine Learning Algorithm to Predict 180-Day Mortality for Outpatients With Cancer.JAMA Oncol. 2020 Nov 1;6(11):1723-1730. doi: 10.1001/jamaoncol.2020.4331. JAMA Oncol. 2020. PMID: 32970131 Free PMC article.
-
Towards proactive palliative care in oncology: developing an explainable EHR-based machine learning model for mortality risk prediction.BMC Palliat Care. 2024 May 20;23(1):124. doi: 10.1186/s12904-024-01457-9. BMC Palliat Care. 2024. PMID: 38769564 Free PMC article.
-
eSyM: An Electronic Health Record-Integrated Patient-Reported Outcomes-Based Cancer Symptom Management Program Used by Six Diverse Health Systems.JCO Clin Cancer Inform. 2022 Jan;6:e2100137. doi: 10.1200/CCI.21.00137. JCO Clin Cancer Inform. 2022. PMID: 34985914 Free PMC article.
-
Machine learning applied to electronic health record data in home healthcare: A scoping review.Int J Med Inform. 2023 Feb;170:104978. doi: 10.1016/j.ijmedinf.2022.104978. Epub 2022 Dec 30. Int J Med Inform. 2023. PMID: 36592572 Free PMC article.
Cited by
-
On the importance of interpretable machine learning predictions to inform clinical decision making in oncology.Front Oncol. 2023 Feb 28;13:1129380. doi: 10.3389/fonc.2023.1129380. eCollection 2023. Front Oncol. 2023. PMID: 36925929 Free PMC article. Review.
-
Design of an interface to communicate artificial intelligence-based prognosis for patients with advanced solid tumors: a user-centered approach.J Am Med Inform Assoc. 2023 Dec 22;31(1):174-187. doi: 10.1093/jamia/ocad201. J Am Med Inform Assoc. 2023. PMID: 37847666 Free PMC article.
-
Uses and limitations of artificial intelligence for oncology.Cancer. 2024 Jun 15;130(12):2101-2107. doi: 10.1002/cncr.35307. Epub 2024 Mar 30. Cancer. 2024. PMID: 38554271 Free PMC article. Review.
-
Use of Patient-Reported Outcomes in Risk Prediction Model Development to Support Cancer Care Delivery: A Scoping Review.JCO Clin Cancer Inform. 2024 Nov;8:e2400145. doi: 10.1200/CCI-24-00145. Epub 2024 Nov 1. JCO Clin Cancer Inform. 2024. PMID: 39486014 Free PMC article.
-
An overview and a roadmap for artificial intelligence in hematology and oncology.J Cancer Res Clin Oncol. 2023 Aug;149(10):7997-8006. doi: 10.1007/s00432-023-04667-5. Epub 2023 Mar 15. J Cancer Res Clin Oncol. 2023. PMID: 36920563 Free PMC article. Review.
References
-
- Paladino J, Bernacki R, Neville BA, et al. Evaluating an intervention to improve communication between oncology clinicians and patients with life-limiting cancer: A cluster randomized clinical trial of the serious illness care program. JAMA Oncol. 2019;5:801–809. - PubMed
-
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non–small-cell lung cancer. N Engl J Med. 2010;363:733–742. - PubMed
-
- Krishnan M, Temel J, Wright A, et al. Predicting life expectancy in patients with advanced incurable cancer: A review. J Support Oncol. 2013;11:68–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
