

Neutralising antibody potency against SARS-CoV-2 wild-type and omicron BA.1 and BA.4/5 variants in patients with inflammatory bowel disease treated with infliximab and vedolizumab after three doses of COVID-19 vaccine (CLARITY IBD): an analysis of a prospective multicentre cohort study
- PMID: 36481043
- PMCID: PMC9757903
- DOI: 10.1016/S2468-1253(22)00389-2
Neutralising antibody potency against SARS-CoV-2 wild-type and omicron BA.1 and BA.4/5 variants in patients with inflammatory bowel disease treated with infliximab and vedolizumab after three doses of COVID-19 vaccine (CLARITY IBD): an analysis of a prospective multicentre cohort study
Abstract
Background: Anti-TNF drugs, such as infliximab, are associated with attenuated antibody responses after SARS-CoV-2 vaccination. We aimed to determine how the anti-TNF drug infliximab and the anti-integrin drug vedolizumab affect vaccine-induced neutralising antibodies against highly transmissible omicron (B.1.1.529) BA.1, and BA.4 and BA.5 (hereafter BA.4/5) SARS-CoV-2 variants, which possess the ability to evade host immunity and, together with emerging sublineages, are now the dominating variants causing current waves of infection.
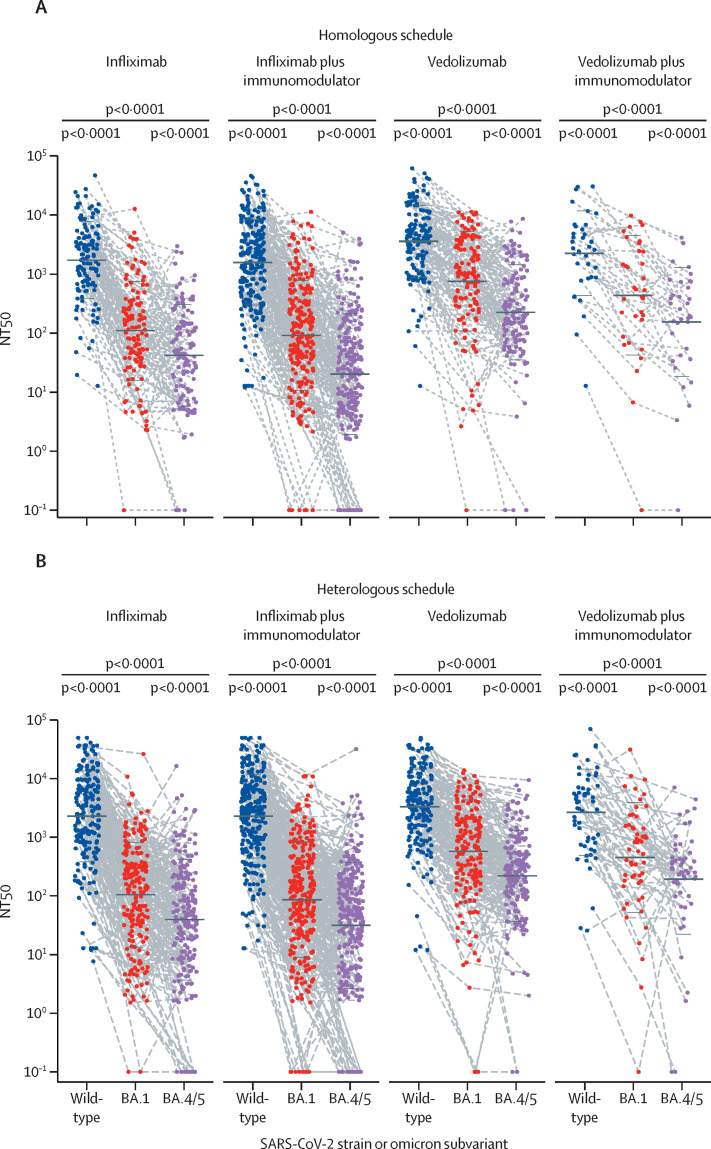
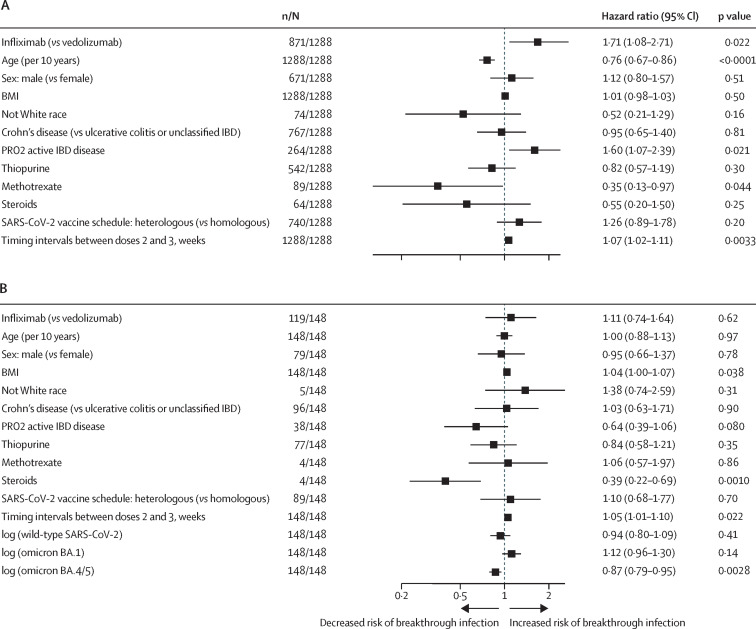
Methods: CLARITY IBD is a prospective, multicentre, observational cohort study investigating the effect of infliximab and vedolizumab on SARS-CoV-2 infection and vaccination in patients with inflammatory bowel disease (IBD). Patients aged 5 years and older with a diagnosis of IBD and being treated with infliximab or vedolizumab for 6 weeks or longer were recruited from infusion units at 92 hospitals in the UK. In this analysis, we included participants who had received uninterrupted biological therapy since recruitment and without a previous SARS-CoV-2 infection. The primary outcome was neutralising antibody responses against SARS-CoV-2 wild-type and omicron subvariants BA.1 and BA.4/5 after three doses of SARS-CoV-2 vaccine. We constructed Cox proportional hazards models to investigate the risk of breakthrough infection in relation to neutralising antibody titres. The study is registered with the ISRCTN registry, ISRCTN45176516, and is closed to accrual.
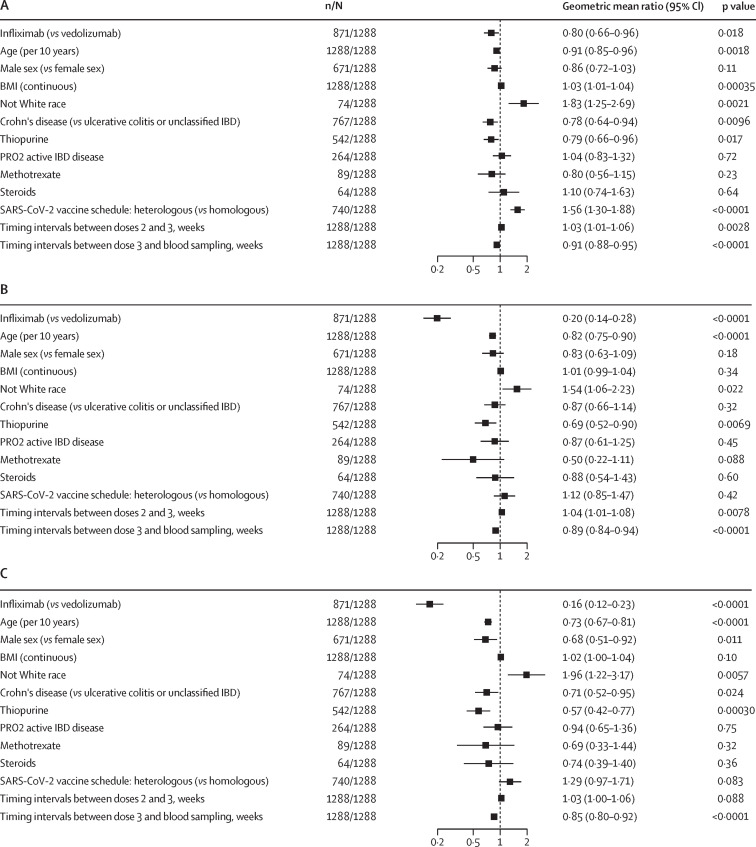
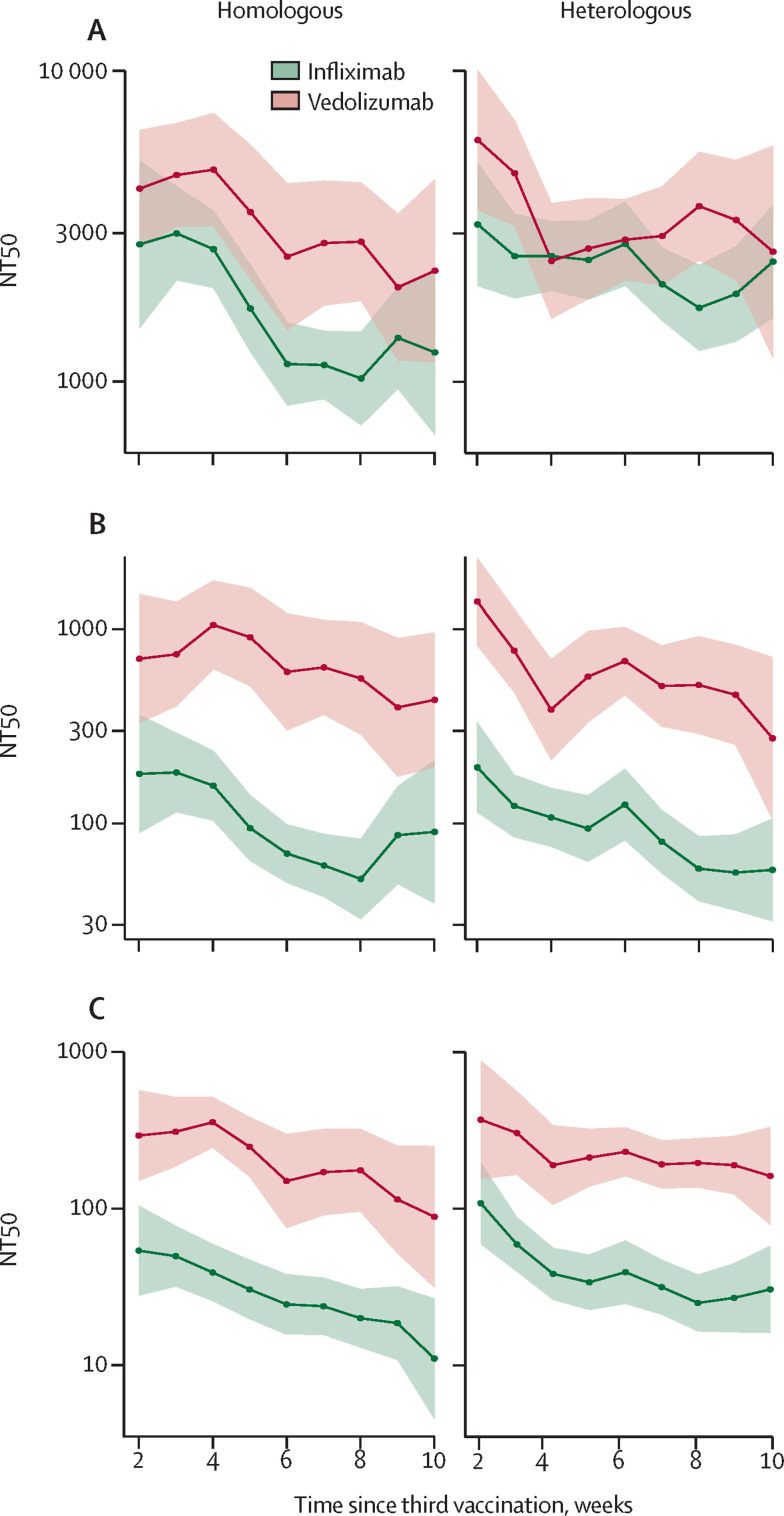
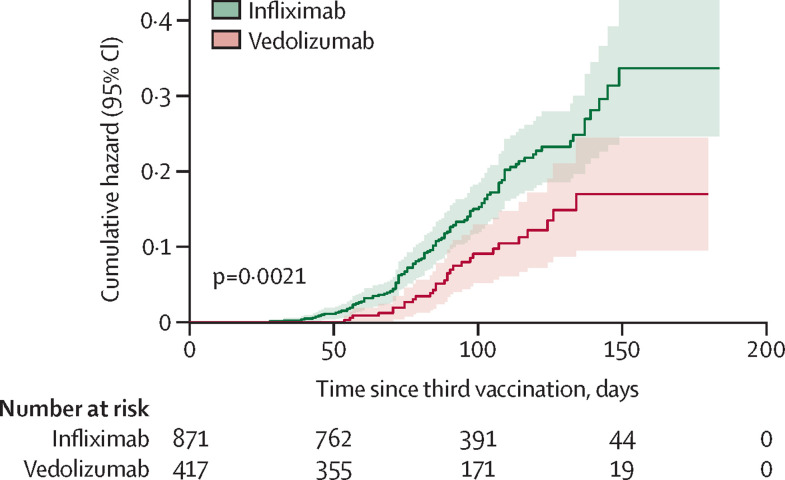
Findings: Between Sept 22 and Dec 23, 2020, 7224 patients with IBD were recruited to the CLARITY IBD study, of whom 1288 had no previous SARS-CoV-2 infection after three doses of SARS-CoV-2 vaccine and were established on either infliximab (n=871) or vedolizumab (n=417) and included in this study (median age was 46·1 years [IQR 33·6-58·2], 610 [47·4%] were female, 671 [52·1%] were male, 1209 [93·9%] were White, and 46 [3·6%] were Asian). After three doses of SARS-CoV-2 vaccine, 50% neutralising titres (NT50s) were significantly lower in patients treated with infliximab than in those treated with vedolizumab, against wild-type (geometric mean 2062 [95% CI 1720-2473] vs 3440 [2939-4026]; p<0·0001), BA.1 (107·3 [86·40-133·2] vs 648·9 [523·5-804·5]; p<0·0001), and BA.4/5 (40·63 [31·99-51·60] vs 223·0 [183·1-271·4]; p<0·0001) variants. Breakthrough infection was significantly more frequent in patients treated with infliximab (119 [13·7%; 95% CI 11·5-16·2] of 871) than in those treated with vedolizumab (29 [7·0% [4·8-10·0] of 417; p=0·00040). Cox proportional hazards models of time to breakthrough infection after the third dose of vaccine showed infliximab treatment to be associated with a higher hazard risk than treatment with vedolizumab (hazard ratio [HR] 1·71 [95% CI 1·08-2·71]; p=0·022). Among participants who had a breakthrough infection, we found that higher neutralising antibody titres against BA.4/5 were associated with a lower hazard risk and, hence, a longer time to breakthrough infection (HR 0·87 [0·79-0·95]; p=0·0028).
Interpretation: Our findings underline the importance of continued SARS-CoV-2 vaccination programmes, including second-generation bivalent vaccines, especially in patient subgroups where vaccine immunogenicity and efficacy might be reduced, such as those on anti-TNF therapies.
Funding: Royal Devon University Healthcare NHS Foundation Trust; Hull University Teaching Hospital NHS Trust; NIHR Imperial Biomedical Research Centre; Crohn's and Colitis UK; Guts UK; National Core Studies Immunity Programme, UK Research and Innovation; and unrestricted educational grants from F Hoffmann-La Roche, Biogen, Celltrion Healthcare, Takeda, and Galapagos.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests SL reports non-financial support from Pfizer and Ferring. SS reports grants from Takeda, Tillots Pharma, Janssen, and Amgen; speaker honoraria from Janssen, Tillotts Pharma, Amgen, AbbVie, and Ferring; personal fees from Takeda, Janssen, and Tillots Pharma; and serving as an advisory board member for Takeda. CAL declares research support or fees for development and delivery of non-promotional education from Janssen, Takeda, AbbVie, AstraZeneca, Eli Lilly, Orion, Pfizer, Roche, Sanofi Aventis, Ferring, Dr Falk, UCB, Biogen, and Genentech. ALH has served as consultant, advisory board member, or speaker for AbbVie, Arena, Atlantic, Bristol-Myers Squibb, Celgene, Celltrion, Falk, Ferring, Galapagos, Janssen, MSD, Napp Pharmaceuticals, Pfizer, Pharmacosmos, Shire, and Takeda and serves on the global steering committee for Genentech. KK reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Janssen and Ferring; support for attending meetings or travel from Janssen and Takeda; and participation on a data safety monitoring board or advisory board for Janssen and PredictImmune. CWL reports personal consulting fees from Galapagos, AbbVie, Takeda, Pfizer, Janssen, and Iterative Scopes; institutional consulting fees from Trellus Health; and personal fees and support for attending meetings from Galapagos, AbbVie, Takeda, Pfizer, Janssen, GSK, Gilead, Fresenius Kabi, Ferring, and Dr Falk. JRG reports grants from F Hoffmann-La Roche, Biogen, Celltrion Healthcare, Takeda, and Galapagos during the study. KMP is chief, principal, or co-investigator for vaccine clinical trials and experimental medicine studies (NCT05007275, NCT04753892, EudraCT 2020-001646-20, NCT04400838, NCT04324606, EudraCT 2017-004610-26, NCT03970993, and NCT03816137), is a member of the data safety monitoring board for two vaccine trials (NCT05249829 and NCT05575492), has received a fee for speaking from Seqirus and Sanofi Pasteur, and has research funding from the Chan Zuckerberg Initiative, the UK Medical research Council/UK Research and Innovation, the Vaccine Task Force, and National Institute for Health Research (NIHR) Imperial Biomedical Research Centre (BRC), outside the submitted work. NAK reports grants from F Hoffmann-La Roche AG, Biogen, Celltrion Healthcare, Takeda, and Galapagos during the conduct of the study; grants and non-financial support from AbbVie, MSD, Napp, Pfizer, Celgene, and Pharmacosmos; grants and personal fees from Celltrion; personal fees and non-financial support from Janssen, Tillots Pharma and Dr Falk; and personal fees from Allergan, Ferring, Pharmacosmos, Takeda, Amgen, Bristol-Myers Squibb, and Mylan, outside the submitted work. TA reports grants from F Hoffmann-La Roche AG, Biogen, Celltrion Healthcare, Takeda, Galapagos, and Crohn's and Colitis UK during the conduct of the study; payment for educational events for Takeda; and serving as medical advisor to Crohn's and Colitis UK, outside of the submitted work. NP reports grants from F Hoffmann-La Roche AG, Biogen, Celltrion Healthcare, Takeda, Galapagos, and Crohn's and Colitis UK during the conduct of the study; research grants from Bristol Myers Squibb and Pfizer; and personal fees from Takeda, Janssen, Pfizer, Galapagos, Bristol-Myers Squibb, AbbVie, Roche, Lilly, Allergan, Celgene, and Astra Zeneca outside the submitted work; and has served as a speaker or advisory board member for AbbVie, Allergan, Bristol-Myers Squibb, Celgene, Dr Falk, Galapagos, AstraZeneca, and Vifor Pharma. SL is supported by a Wellcome GW4-CAT fellowship. NC acknowledges support from Crohn's and Colitis UK. CAL acknowledges support from the NIHR Newcastle BRC and the support of the Programmed Investigation Unit at Royal Victoria Infirmary, Newcastle upon Tyne. CWL is funded by a UKRI Future Leaders Fellowship. NP is supported by the NIHR Imperial BRC. All other authors declare no competing interests.
Figures
Comment in
-
Working towards a comprehensive appraisal of vaccine-induced immunity against SARS-CoV-2 in IBD.Lancet Gastroenterol Hepatol. 2023 Feb;8(2):99-100. doi: 10.1016/S2468-1253(22)00404-6. Epub 2022 Dec 5. Lancet Gastroenterol Hepatol. 2023. PMID: 36481042 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
