

Bilateral persistent intersegmental artery in a patient with posterior atlantoaxial subluxation after subaxial cervical laminoplasty
- PMID: 36481588
- PMCID: PMC9731870
- DOI: 10.1016/j.ijscr.2022.107796
Bilateral persistent intersegmental artery in a patient with posterior atlantoaxial subluxation after subaxial cervical laminoplasty
Abstract
Introduction and importance: To summarize the clinical manifestations and treatment of bilateral persistent first intersegmental artery (PFIA) in a patient with posterior subluxation of atlantoaxial joint.
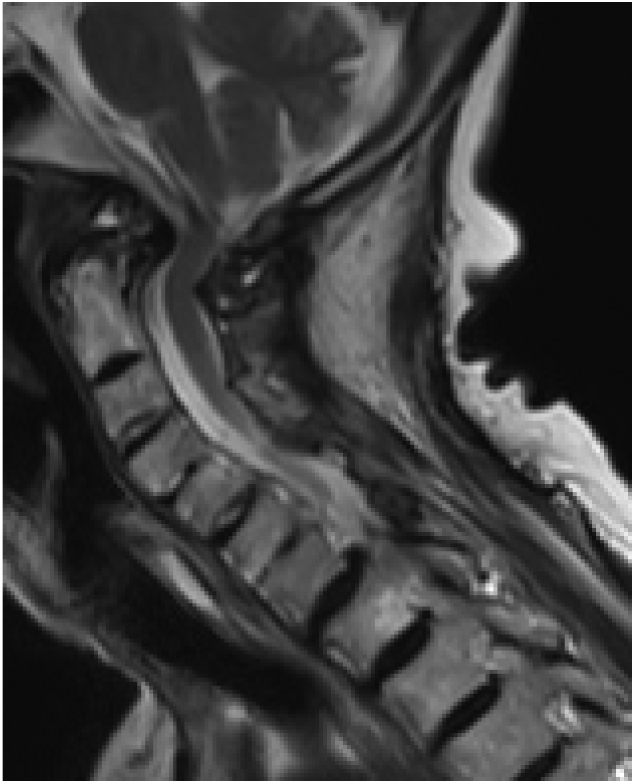
Case presentation: A-85-year-old woman with a two-months history of aggravating of gait disturbance and finger clumsiness was referred to our hospital. Magnetic resonance imaging revealed posterior subluxation of the atlantoaxial joint and spinal cord compression at C1 level. Three-dimensional computed tomography angiography (CTA) of cervical spine showed bilateral PFIA and left side high-riding VA. Because of the high risk of vertebral artery injury with posterior arch resection and lateral mass screw insertion due to the presence of PFIA, as well as the bony fragility of the cervical spine and the fact that the posterior atlantoaxial subluxation was reduced in the flexed position, the posterior occipito-thoracic fixation without posterior arch resection in the mildly flexed cervical position was underwent. The postoperative course was uneventful and her neurological symptoms improved gradually after surgery.
Clinical discussion: PFIA is a very rare condition representing between 0.01 % and 1.8 %. Most patients with this condition have a unilateral persistent segmental artery, but in a small minority of cases it occurs bilaterally. It may be more difficult to resect of posterior arch or insert the C1 lateral mass screw in cases of PFIA.
Conclusion: The best way to avoid IVAI may be careful examining the abnormal running of VA preoperatively especially on 3D-CT of cervical spine with arteriography and not to choose a technique with a high risk of VA injury.
Keywords: Atlantoaxial subluxation; Bilateral persistent first intersegmental artery; Cervical spondylotic myelopathy; High riding vertebral artery; Iatrogenic vertebral artery injury; Occipitothoracic fixation.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest This work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Maughan P.H., Elhadi A.M., Martirosyan N.L., et al. Multimodality management of vertebral artery injury susutained during cervical or craniocervical surgery. Oper. Neurosurg. 2013;73:271–282. - PubMed
-
- Lunardini D.J., Eskander M.S., Even J.L., et al. Vertebral artery injuries in cervical spine surgery. Spine J. 2014;14:1520–1525. - PubMed
-
- Lee C.H., Hong J.T., Kang D.H., et al. Epidemiology of iatrogenic vertebral artery injury in cervical spine surgery:21 multicenter studies. World Neurosurg. 2019;126:e1050–e1054. - PubMed
-
- Yamazaki M., Okawa A., Furuya T., et al. Anomalous vertebral arteries in the extra- and intraosseous regions of the craniovertebral junction visualized by 3-dimensional computed tomographic angiography. Spine. 2012;37:E1389–E1397. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
