

A model established for predicting natural pregnancy possibility based on the imaging characteristics of 4-dimensional hysterosalpingo-contrast sonography
- PMID: 36481639
- PMCID: PMC10930629
- DOI: 10.11817/j.issn.1672-7347.2022.220179
A model established for predicting natural pregnancy possibility based on the imaging characteristics of 4-dimensional hysterosalpingo-contrast sonography
Abstract
Objectives: The incidence of infertility is increasing, more than 30% of them having related abnormal tubal patency. Four-dimensional (4D) hysterosalpingo-contrast sonography (HyCoSy) overcomes the shortcomings of 3D HyCoSy in the diagnosis of tubal patency, showing high specificity and accuracy. In addition, 4D HyCoSy discards iodine allergy and X-ray radiation and possesses easy-operating, contributing to good acceptance in clinical practice. However, there is no research to explore the imaging standards related to the possibility of natural pregnancy after 4D HyCoSy. If a predictive model of postoperative natural pregnancy was established using the analysis of clinical data combined with imaging characteristics of 4D HyCoSy of patients with tubal factor infertility, clinical decision-making can be wisely guided in the future. This study aims to establish a predictive model of natural pregnancy after 4D HyCoSy based on clinical data and imaging characteristics of patients with tubal factor in fertility.
Methods: A retrospective study was conducted for patients who were diagnosed with tubal factor infertility in Hunan Guangxiu Hospital from February 2017 to May 2018. The patients ought to possess complete 4D HyCoSy imaging data and at least one-side-unobstructed fallopian tube. General clinical data and imaging data were collected. Pregnancy outcome was followed up till 3 months after 4D HyCoSy. According to pregnancy outcome, patients were divided into a pregnancy group and a non-pregnancy group. Binary logistic regression was used to analyze the correlation between various variables and natural pregnancy after 4D HyCoSy. The variables with significant difference (P<0.05) in single-factor logistic regression were included in the natural pregnancy probability prediction model. The classification accuracy was further verified with 10-fold cross-validation.
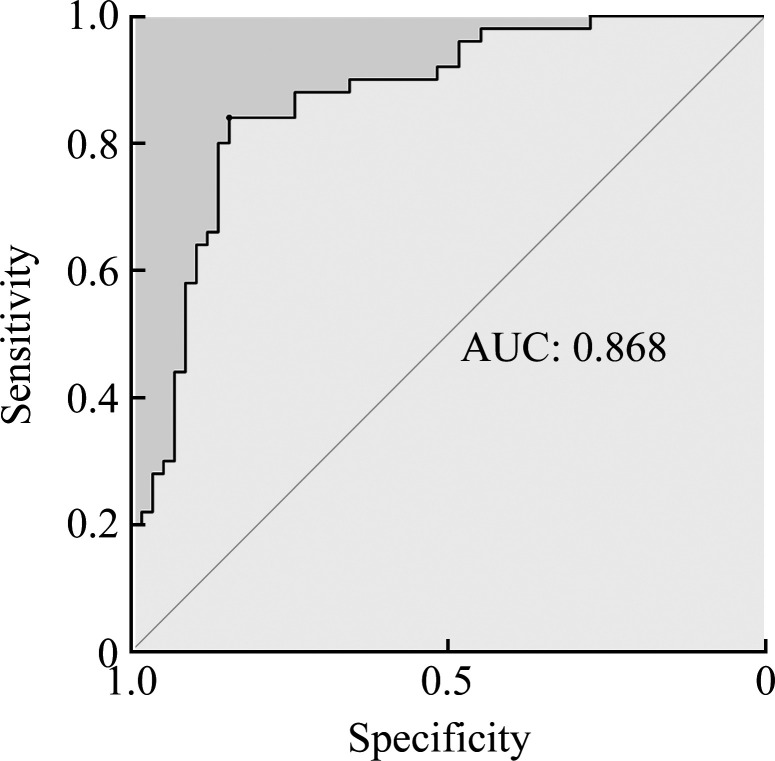
Results: A total of 1 085 patients with clinically suspected tubal factor infertility who met the requirements and followed the doctors' prescription were collected. Clinical characteristics (age and duration of infertility) and 4D HyCoSy imaging characteristics (thickness of endometrium from the 3rd to the 7th day after the end of menstruation, visualization of the left fallopian tube, the diffusion of contrast agent around the left ovary, and the diffusion of contrast agent around the right ovary) were independent predictors for natural pregnancy 3 months after 4D HyCoSy. A natural pregnancy probability prediction model was established with the area under the curve (AUC) verified by the 10-fold cross-validation all greater than 0.75, and the best AUC was 0.868. The Q value obtained by the prediction model was the probability of natural pregnancy, and the cutoff value was 0.5. When the Q value was greater than 0.5, it was recommended to attempt natural pregnancy for 3 months, and when the Q value was less than 0.5, in vitro fertilization was adviced.
Conclusions: A predictive model for the evaluating probability of natural pregnancy in women with tubal factor infertility after 4D HyCoSy is successfully established based on the analysis for clinical data and imaging characteristics. This model shows a great potential in assisting clinical decision making.
目的: 不孕症的发病率呈逐年上升的趋势,其中30%以上与输卵管通畅性异常相关。四维超声子宫输卵管造影(4-dimensional hysterosalpingo-contrast sonography,4D HyCoSy)在诊断输卵管通畅性上既克服了三维成像的不足,特异性和准确性均较高,又避免了碘剂过敏、X线辐射等危害,接受度好且易掌握,在临床应用越来越广泛,但是目前尚无研究探讨4D HyCoSy与自然妊娠可能性相关的影像学标准。本研究对临床拟诊输卵管性不孕患者的临床资料及4D HyCoSy的影像特点进行分析,建立一种基于影像学特征的造影术后自然妊娠的预测模型。方法: 回顾性分析湖南省光琇医院2017年2月至2018年5月拟诊为输卵管性不孕症、具有完整4D HyCoSy影像学资料且显示至少一侧输卵管通畅的患者,收集患者的一般临床资料及影像数据,并随访患者造影术后3个月内的自然妊娠情况,将其分成自然妊娠组与非自然妊娠组。采用二元logistic回归分析各个变量与造影术后自然妊娠之间的相关性,将单因素logistic回归中差异有统计学意义(P<0.05)的变量纳入自然妊娠概率预测模型,并通过10倍交叉法验证预测模型的分类能力。结果: 收集到符合要求且遵医嘱试孕3个月的1 085名临床拟诊输卵管性不孕患者,其临床特征(年龄、不孕年限)及4D HyCoSy影像学特征(月经结束后3~7 d的内膜厚度、左侧输卵管显影情况、左侧卵巢周围造影剂弥散情况、右侧卵巢周围造影剂弥散情况)是术后3个月自然妊娠的独立预测因素。建立自然妊娠概率预测模型,10倍交叉法验证得出的曲线下面积(area under the curve,AUC)均大于0.75,最佳AUC为0.868。预测模型得出的Q值为自然妊娠概率,截断值是0.5,当Q值大于0.5时建议试孕3个月,小于0.5时建议采用辅助生殖技术助孕。结论: 基于输卵管性不孕患者的临床及4D HyCoSy的影像学特征成功建立了输卵管性不孕症女性造影术后自然妊娠的预测模型,此模型可有效辅助临床进行个体化决策。.
Keywords: four-dimensional hysterosalpingo-contrast sonography; infertility; natural pregnancy; predictive model; tubal patency.
Conflict of interest statement
作者声称无任何利益冲突。
Figures
Similar articles
-
The value of transvaginal 4-dimensional hysterosalpingo-contrast sonography in predicting the necessity of assisted reproductive technology for women with tubal factor infertility.Quant Imaging Med Surg. 2021 Aug;11(8):3698-3714. doi: 10.21037/qims-20-1193. Quant Imaging Med Surg. 2021. PMID: 34341743 Free PMC article.
-
Spontaneous conception outcome in infertile women after four-dimensional hysterosalpingo-contrast-sonography.BMC Pregnancy Childbirth. 2020 Oct 20;20(1):638. doi: 10.1186/s12884-020-03315-x. BMC Pregnancy Childbirth. 2020. PMID: 33081754 Free PMC article.
-
Diagnostic value of transvaginal four-dimensional hysterosalpingo-contrast sonography combined with recanalization in patients with tubal infertility.Niger J Clin Pract. 2019 Jan;22(1):46-50. doi: 10.4103/njcp.njcp_376_17. Niger J Clin Pract. 2019. PMID: 30666019
-
Two-dimensional hysterosalpingo-contrast-sonography compared to three/four-dimensional hysterosalpingo-contrast-sonography for the assessment of tubal occlusion in women with infertility/subfertility: a systematic review with meta-analysis.Hum Fertil (Camb). 2022 Feb;25(1):43-55. doi: 10.1080/14647273.2020.1769204. Epub 2020 Jun 2. Hum Fertil (Camb). 2022. PMID: 32484066
-
Hysterosalpingo-contrast-sonography vs. magnetic resonance-hysterosalpingography for diagnosing fallopian tubal patency: A systematic review and meta-analysis.Eur J Radiol. 2020 Apr;125:108891. doi: 10.1016/j.ejrad.2020.108891. Epub 2020 Feb 20. Eur J Radiol. 2020. PMID: 32088657
Cited by
-
Evaluation of tubal patency based on peak injection pressure in four-dimensional hysterosalpingo-contrast sonography among infertile females: a preliminary study.Quant Imaging Med Surg. 2024 May 1;14(5):3461-3472. doi: 10.21037/qims-23-1569. Epub 2024 Apr 26. Quant Imaging Med Surg. 2024. PMID: 38720834 Free PMC article.
References
-
- He YN, Ma XH, Xu JJ, et al. . Comparison of assessment methods for fallopian tubal patency and peritubal adhesion between transvaginal 4-dimensional hysterosalpingo-contrast sonography and laparoscopic chromopertubation[J]. J Ultrasound Med, 2017, 36(3): 547-556. 10.7863/ultra.15.11056. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
