

First-line options for systemic juvenile idiopathic arthritis treatment: an observational study of Childhood Arthritis and Rheumatology Research Alliance Consensus Treatment Plans
- PMID: 36482434
- PMCID: PMC9730566
- DOI: 10.1186/s12969-022-00768-6
First-line options for systemic juvenile idiopathic arthritis treatment: an observational study of Childhood Arthritis and Rheumatology Research Alliance Consensus Treatment Plans
Abstract
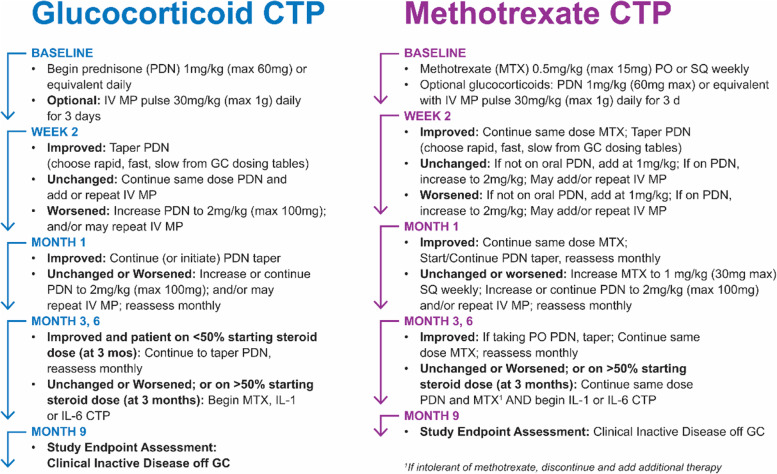
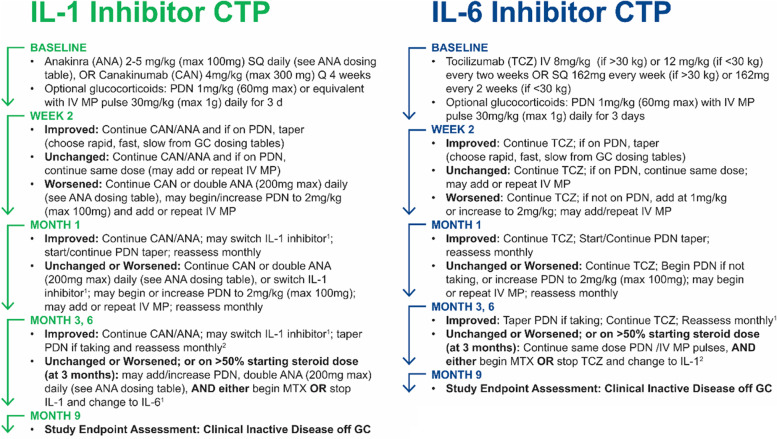
Background: The Childhood Arthritis and Rheumatology Research Alliance (CARRA) developed consensus treatment plans (CTPs) to compare treatment initiation strategies for systemic juvenile idiopathic arthritis (sJIA). First-line options for sJIA treatment (FROST) was a prospective observational study to assess CTP outcomes using the CARRA Registry.
Methods: Patients with new-onset sJIA were enrolled if they received initial treatment according to the biologic CTPs (IL-1 or IL-6 inhibitor) or non-biologic CTPs (glucocorticoid (GC) monotherapy or methotrexate). CTPs could be used with or without systemic GC. Primary outcome was achievement of clinical inactive disease (CID) at 9 months without current use of GC. Due to the small numbers of patients in the non-biologic CTPs, no statistical comparisons were made between the CTPs.
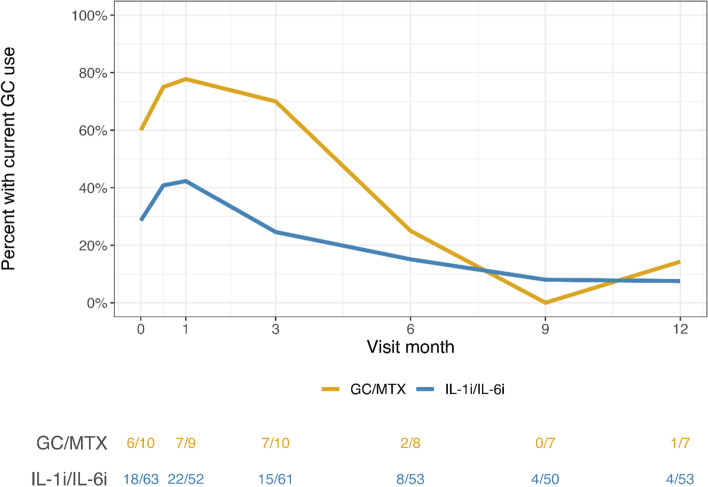
Results: Seventy-three patients were enrolled: 63 (86%) in the biologic CTPs and 10 (14%) in the non-biologic CTPs. CTP choice appeared to be strongly influenced by physician preference. During the first month of follow-up, oral GC use was observed in 54% of biologic CTP patients and 90% of non-biologic CTPs patients. Five (50%) non-biologic CTP patients subsequently received biologics within 4 months of follow-up. Overall, 30/53 (57%) of patients achieved CID at 9 months without current GC use.
Conclusion: Nearly all patients received treatment with biologics during the study period, and 46% of biologic CTP patients did not receive oral GC within the first month of treatment. The majority of patients had favorable short-term clinical outcomes. Increased use of biologics and decreased use of GC may lead to improved outcomes in sJIA.
Keywords: Biologics; Juvenile idiopathic arthritis; Still’s disease; Systemic juvenile idiopathic arthritis; Treatment.
© 2022. The Author(s).
Conflict of interest statement
TB has received consulting fees from Novartis and UCB. PAN receives investigator-initiated research grants from Bristol-Myers Squibb and Pfizer; consulting from Bristol-Myers Squibb, Cerecor, Exo Therapeutics, Miach Orthopedics, Novartis, and Pfizer; royalties from UpToDate Inc.; and salary support from the Childhood Arthritis and Rheumatology Research Alliance. LES has received research support from Bristol-Myers Squibb. LES serves on the data and safety monitoring board for Sanofi (sarilumab) and UCB (certolizumab). SM and EP are employees and shareholders of Genentech, Inc. YK has received research support from Genentech.
Figures
References
-
- Kimura Y, Vastert S. Systemic juvenile idiopathic arthritis (chapter 17) In: Petty RE, Laxer RM, Lindsley CB, Wedderburn LR, Mellins ED, Fuhlbrigge RC, editors. Textbook of pediatric rheumatology. 8. Philadelphia: Elsevier, Inc.; 2021.
-
- Quartier P, Allantaz F, Cimaz R, Pillet P, Messiaen C, Bardin C, et al. A multicentre, randomised, double-blind, placebo-controlled trial with the interleukin-1 receptor antagonist anakinra in patients with systemic-onset juvenile idiopathic arthritis (ANAJIS trial) Ann Rheum Dis. 2011;70(5):747–754. doi: 10.1136/ard.2010.134254. - DOI - PMC - PubMed
-
- Nigrovic PA, Mannion M, Prince FH, Zeft A, Rabinovich CE, van Rossum MA, et al. Anakinra as first-line disease-modifying therapy in systemic juvenile idiopathic arthritis: report of forty-six patients from an international multicenter series. Arthritis Rheum. 2011;63(2):545–555. doi: 10.1002/art.30128. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
