

Refeeding Syndrome
- PMID: 36482748
- PMCID: PMC10132284
- DOI: 10.3238/arztebl.m2022.0381
Refeeding Syndrome
Abstract
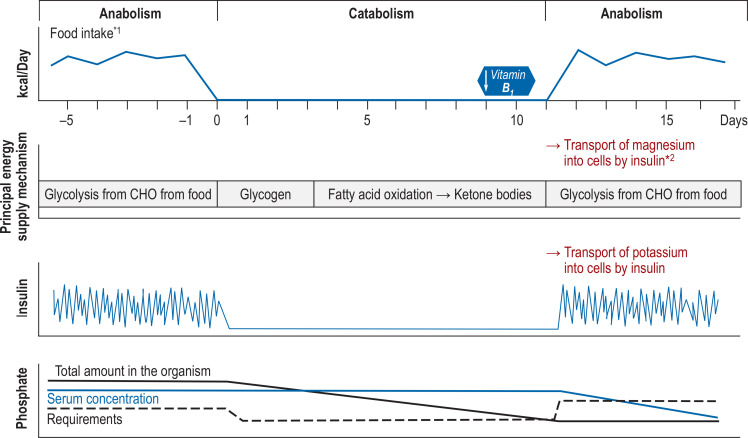
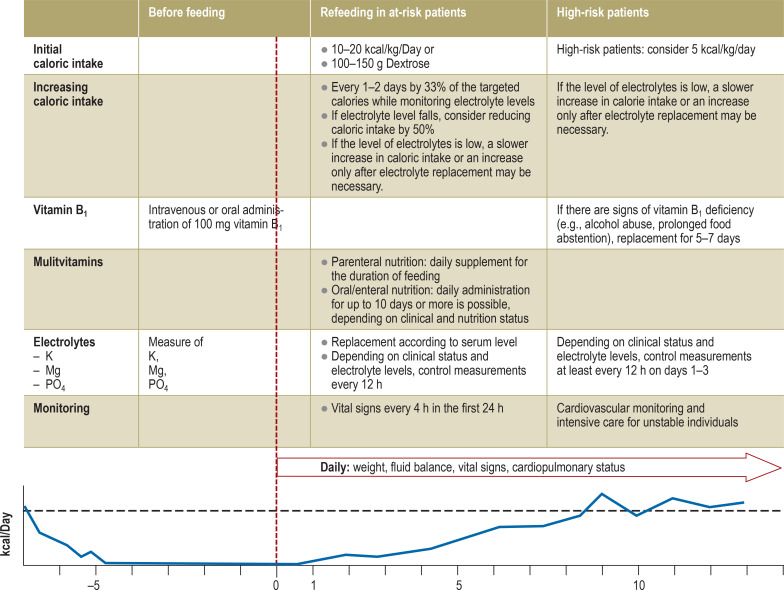
Background: Refeeding syndrome (RFS) can occur in malnourished patients when normal, enteral, or parenteral feeding is resumed. The syndrome often goes unrecognized and may, in the most severe cases, result in death. The diagnosis of RFS can be crucially facilitated by the use of clinical decision support systems (CDSS).
Methods: The literature in PubMed was searched for current treatment recommendations, randomized intervention studies, and publications on RFS and CDSS. We also took account of insights gained from the development and implementation of our own CDSS for the diagnosis of RFS.
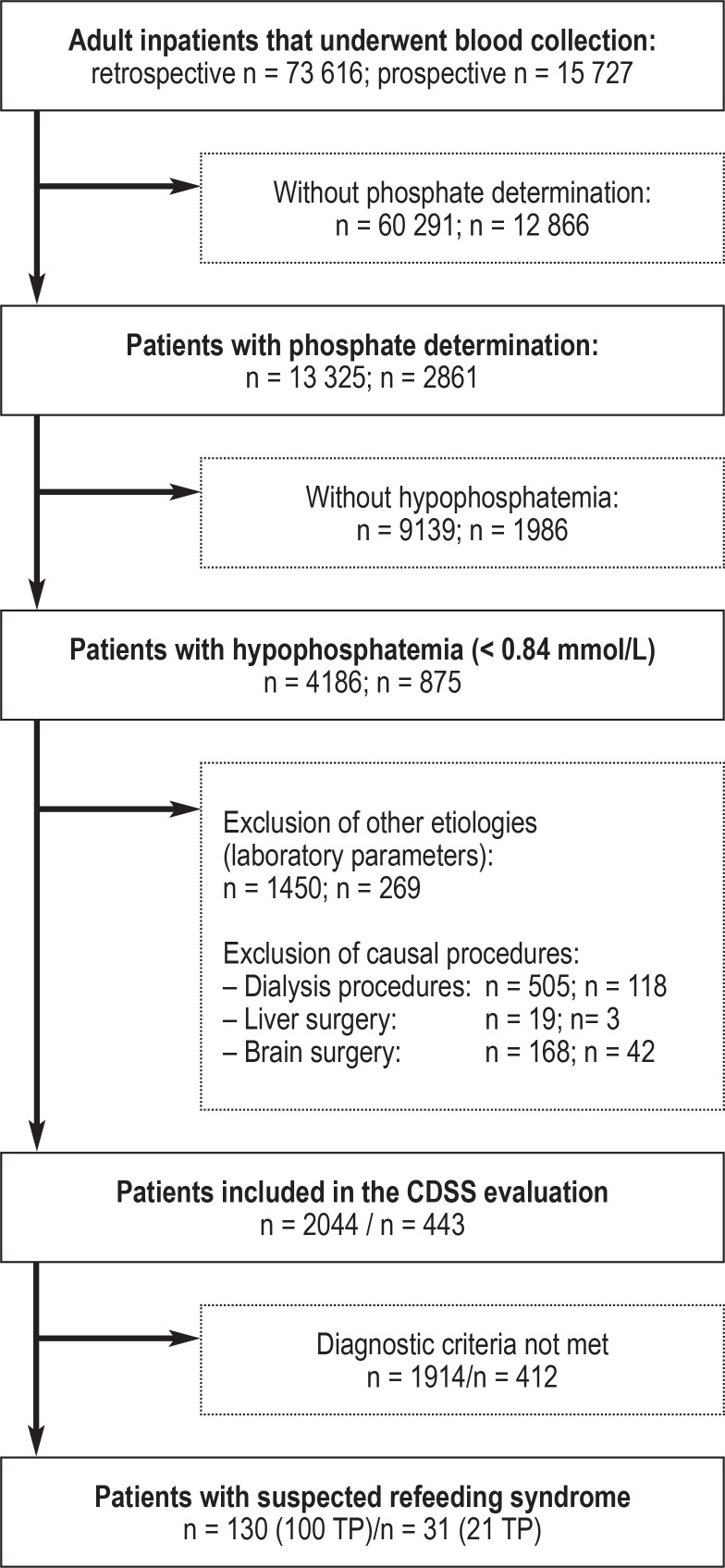
Results: The identification of high-risk patients and the recognition of manifest RFS is clinically challenging due to the syndrome's unspecific symptoms and physicians' lack of awareness of the risk of this condition. The literature shows that compared to patients without RFS, malnourished patients with RFS have significantly greater 6-month mortality (odds ratio 1.54, 95% confidence interval: [1.04; 2.28]) and an elevated risk of admission to intensive care (odds ratio 2.71 [1.01; 7.27]). In a prospective testing program, use of our own CDSS led to correct diagnosis in two thirds of cases.
Conclusion: RFS is difficult to detect and represents a high risk to the patients affected. Appropriate CDSS can identify such patients and ensure proper professional care.
Figures
References
-
- Zeki S, Culkin A, Gabe SM, Nightingale JM. Refeeding hypophosphataemia is more common in enteral than parenteral feeding in adult in patients. Clin Nutr. 2011;30:365–368. - PubMed
-
- da Silva JSV, Seres DS, Sabino K, et al. ASPEN Consensus recommendations for refeeding syndrome. Nutr Clin Pract. 2020;35:178–195. - PubMed
-
- Janssen G, Pourhassan M, Lenzen-Großimlinghaus R, et al. The refeeding syndrome revisited: you can only diagnose what you know. Eur J Clin Nutr. 2019;73:1458–1463. - PubMed
-
- Larsen S. The investigation of parenteral nutrition - Aotearoa (IPNA) setting up the 1st phase of a clinical audit of the delivery of parenteral nutrition (PN) in New Zealand (NZ) Masterarbeit. Albany, New Zealand. 2012
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical