

This is a preprint.
SARS-CoV-2 Vaccine Booster Elicits Robust Prolonged Maternal Antibody Responses and Passive Transfer Via The Placenta And Breastmilk
- PMID: 36482972
- PMCID: PMC9727762
- DOI: 10.1101/2022.11.29.518385
SARS-CoV-2 Vaccine Booster Elicits Robust Prolonged Maternal Antibody Responses and Passive Transfer Via The Placenta And Breastmilk
Update in
-
SARS-CoV-2 vaccine booster elicits robust prolonged maternal antibody responses and passive transfer to the offspring via the placenta and breastmilk.Am J Obstet Gynecol MFM. 2023 Feb;5(2):100830. doi: 10.1016/j.ajogmf.2022.100830. Epub 2022 Nov 30. Am J Obstet Gynecol MFM. 2023. PMID: 36462615 Free PMC article. No abstract available.
Abstract
Background: Infection during pregnancy can result in adverse outcomes for both pregnant persons and offspring. Maternal vaccination is an effective mechanism to protect both mother and neonate into post-partum. However, our understanding of passive transfer of antibodies elicited by maternal SARS-CoV-2 mRNA vaccination during pregnancy remains incomplete.
Objective: We aimed to evaluate the antibody responses engendered by maternal SARS-CoV-2 vaccination following initial and booster doses in maternal circulation and breastmilk to better understand passive immunization of the newborn.
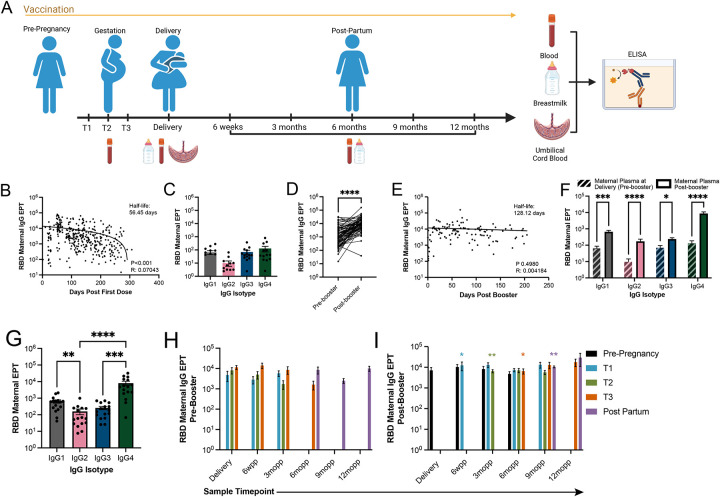
Study design: We collected longitudinal blood samples from 121 pregnant women who received SARS-CoV-2 mRNA vaccines spanning from early gestation to delivery followed by collection of blood samples and breastmilk between delivery and 12 months post-partum. During the study, 70% of the participants also received a booster post-partum. Paired maternal plasma, breastmilk, umbilical cord plasma, and newborn plasma samples were tested via enzyme-linked immunosorbent assays (ELISA) to evaluate SARS-CoV-2 specific IgG antibody levels.
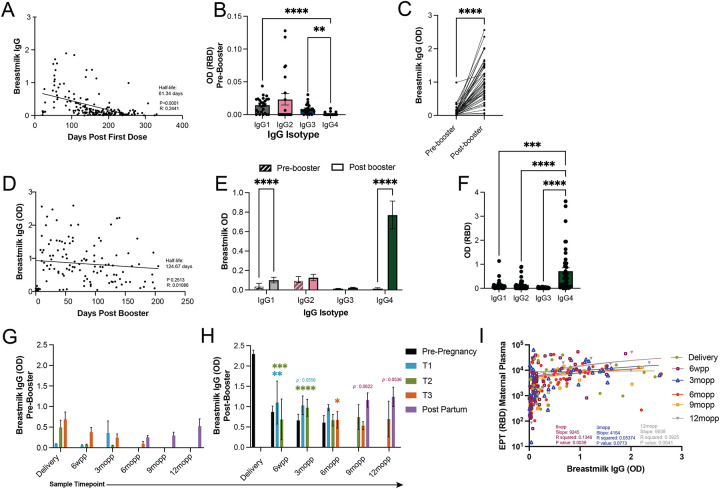
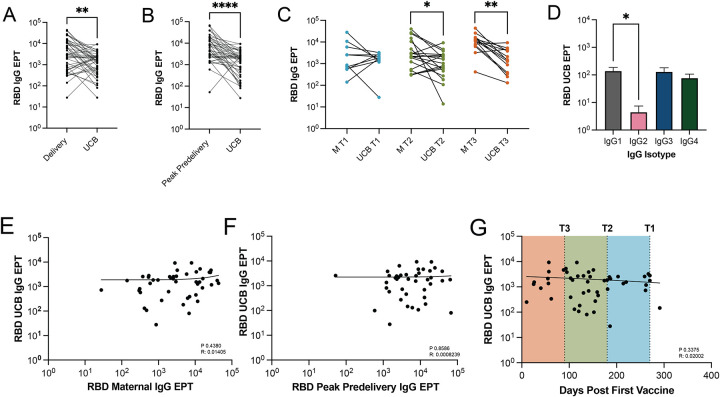
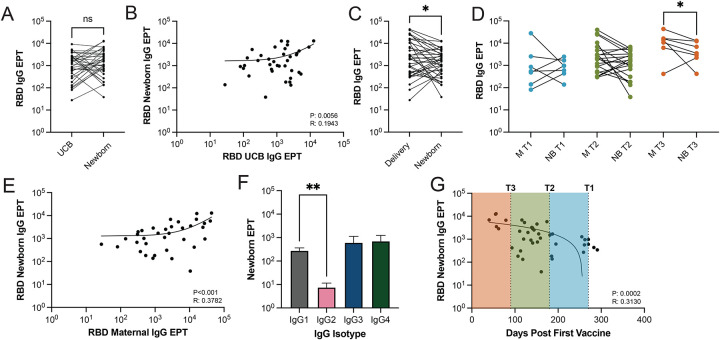
Results: Vaccine-elicited maternal antibodies were detected in both cord blood and newborn blood, albeit at lower levels than maternal circulation, demonstrating transplacental passive immunization. Booster vaccination significantly increased spike specific IgG antibody titers in maternal plasma and breastmilk. Finally, SARS-CoV-2 specific IgG antibodies in newborn blood correlated negatively with days post initial maternal vaccine dose.
Conclusion: Vaccine-induced maternal SARS-CoV-2 antibodies were passively transferred to the offspring in utero via the placenta and after birth via breastfeeding. Maternal booster vaccination, regardless of gestational age at maternal vaccination, significantly increased antibody levels in breastmilk and maternal plasma, indicating the importance of this additional dose to maximize passive protection against SARS-CoV-2 infection for neonates and infants until vaccination eligibility.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Association of Gestational Age at Coronavirus Disease 2019 (COVID-19) Vaccination, History of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection, and a Vaccine Booster Dose With Maternal and Umbilical Cord Antibody Levels at Delivery.Obstet Gynecol. 2022 Mar 1;139(3):373-380. doi: 10.1097/AOG.0000000000004693. Obstet Gynecol. 2022. PMID: 34963127
-
COVID-19 booster vaccination during pregnancy enhances maternal binding and neutralizing antibody responses and transplacental antibody transfer to the newborn (DMID 21-0004).medRxiv [Preprint]. 2022 Jun 13:2022.06.13.22276354. doi: 10.1101/2022.06.13.22276354. medRxiv. 2022. Update in: Vaccine. 2023 Aug 14;41(36):5296-5303. doi: 10.1016/j.vaccine.2023.06.032. PMID: 35734087 Free PMC article. Updated. Preprint.
-
Maternal and Neonatal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Immunoglobulin G Levels After the Pfizer-BioNTech Booster Dose for Coronavirus Disease 2019 (COVID-19) Vaccination During the Second Trimester of Pregnancy.Obstet Gynecol. 2022 Aug 1;140(2):187-193. doi: 10.1097/AOG.0000000000004867. Epub 2022 May 27. Obstet Gynecol. 2022. PMID: 35852268
-
Role of maternal COVID-19 vaccination in providing immunological protection to the newborn.Pharmacotherapy. 2022 Jan;42(1):58-70. doi: 10.1002/phar.2649. Epub 2021 Dec 15. Pharmacotherapy. 2022. PMID: 34816467 Review.
-
Impact of Infections During Pregnancy on Transplacental Antibody Transfer.Vaccines (Basel). 2024 Oct 21;12(10):1199. doi: 10.3390/vaccines12101199. Vaccines (Basel). 2024. PMID: 39460363 Free PMC article. Review.
Cited by
-
Built environment microbiomes transition from outdoor to human-associated communities after construction and commissioning.Sci Rep. 2023 Sep 22;13(1):15854. doi: 10.1038/s41598-023-42427-0. Sci Rep. 2023. PMID: 37740013 Free PMC article.
References
-
- Levy O. Innate immunity of the human newborn: distinct cytokine responses to LPS and other Toll-like receptor agonists. J Endotoxin Res 2005;11:113–6. - PubMed
-
- Clapp DW. Developmental regulation of the immune system. Semin Perinatol 2006;30:69–72. - PubMed
-
- Organization WH. Newborn Mortality 2022.
-
- World Health O. Neonatal and perinatal mortality: country, regional and global estimates. Geneva: World Health Organization, 2006.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous