

Understanding healthcare provider preferences for ordering respiratory cultures to diagnose ventilator associated pneumonia: A discrete choice experiment
- PMID: 36483413
- PMCID: PMC9726546
- DOI: 10.1017/ash.2022.267
Understanding healthcare provider preferences for ordering respiratory cultures to diagnose ventilator associated pneumonia: A discrete choice experiment
Abstract
Objective: Ventilator-associated pneumonia (VAP) can be overdiagnosed on the basis of positive respiratory cultures in the absence of clinical findings of pneumonia. We determined the perceived diagnostic importance of 6 clinical attributes in ordering a respiratory culture to identify opportunities for diagnostic stewardship.
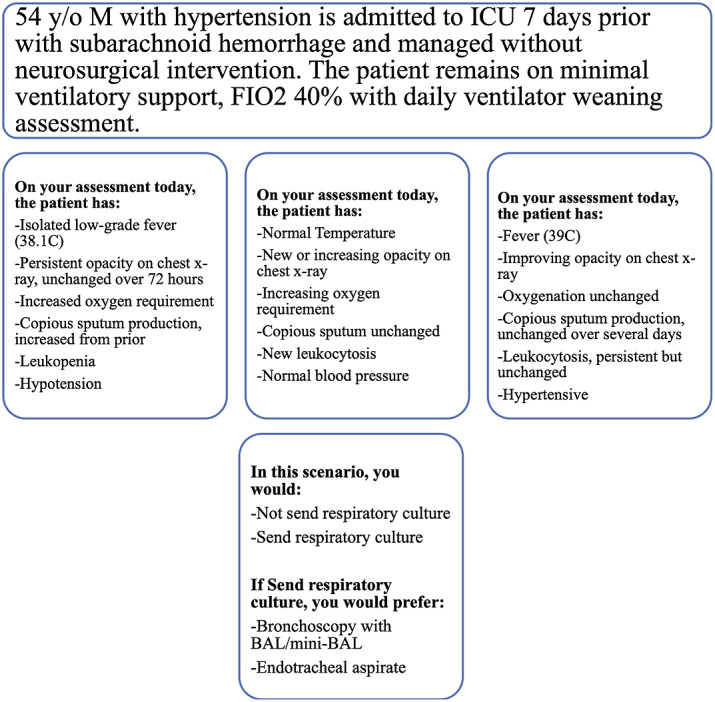
Design: A discrete choice experiment presented participants with a vignette consisting of the same "stem" plus variations in 6 clinical attributes associated with VAP: chest imaging, oxygenation, sputum, temperature, white blood cell count, and blood pressure. Each attribute had 3-4 levels, resulting in 32 total scenarios. Participants indicated whether they would order a respiratory culture, and if yes, whether they preferred the bronchoalveolar lavage or endotracheal aspirate sample-collection method. We calculated diagnostic utility of attribute levels and relative importance of each attribute.
Setting and participants: The survey was administered electronically to critical-care clinicians via a Qualtrics survey at a tertiary-care academic center in the United States.
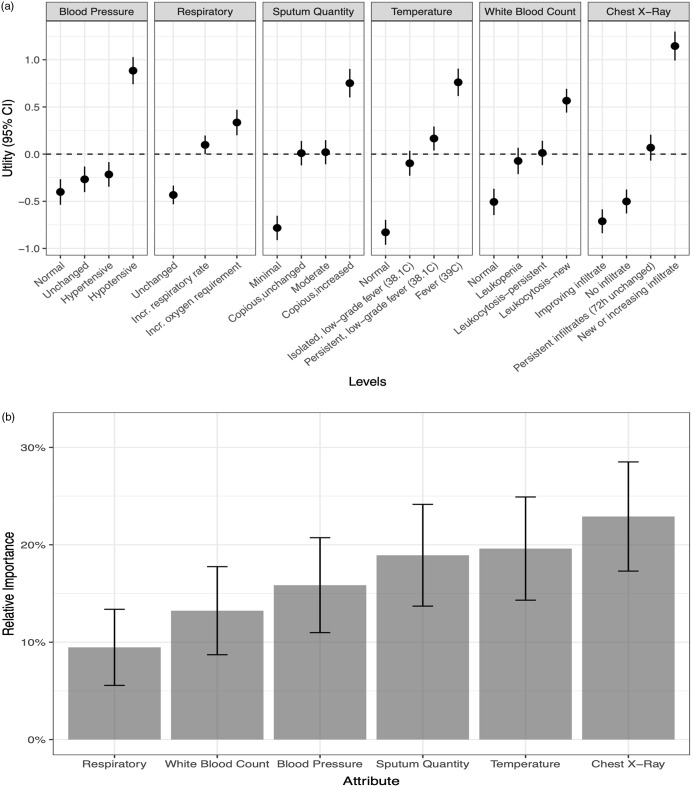
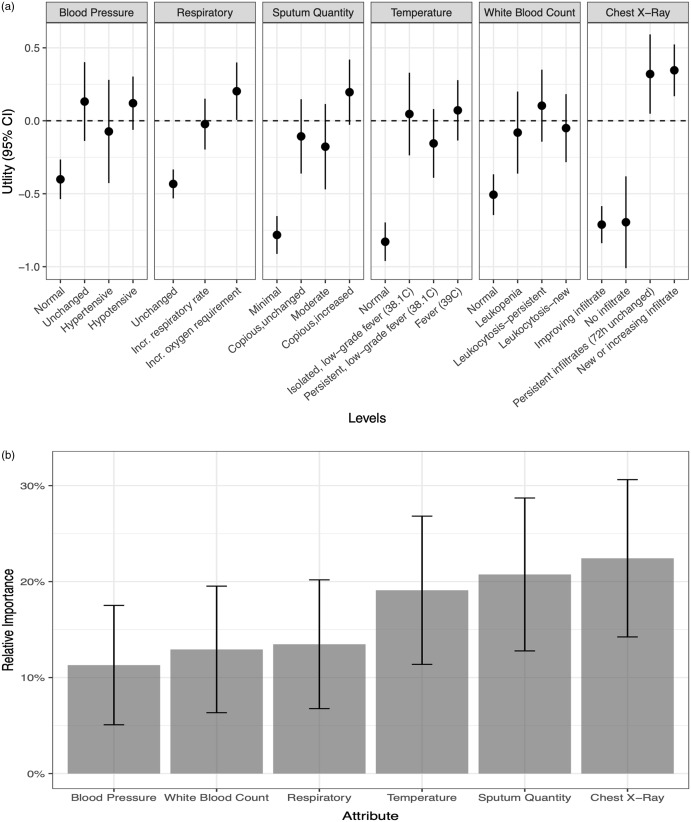
Results: In total, 59 respondents completed the survey. New radiograph opacity (utility, 1.15; 95% confidence interval [CI], 0.99-1.3), hypotension (utility, 0.88; 95% CI, 0.74-1.03), fever (utility, 0.76; 95% CI, 0.62-0.91) and copious sputum (utility, 0.75; 95% CI, 0.60-0.90) had the greatest perceived diagnostic value that favored ordering a respiratory culture. Radiograph changes (23%) and temperature (20%) had the highest relative importance. New opacity (utility, 0.35; 95% CI, 0.17-0.52) and persistent opacity on radiograph (utility, 0.32; 95% CI, 0.05-0.59) had the greatest value favoring bronchoalveolar lavage over endotracheal aspirate.
Conclusion: Perceived high diagnostic value of fever and hypotension suggest that sepsis vigilance may drive respiratory culturing and play a role in VAP overdiagnosis.
© The Author(s) 2022.
Figures
Similar articles
-
Healthcare providers consistently overestimate the diagnostic probability of ventilator-associated pneumonia.Infect Control Hosp Epidemiol. 2023 Dec;44(12):1927-1931. doi: 10.1017/ice.2023.62. Epub 2023 Jun 23. Infect Control Hosp Epidemiol. 2023. PMID: 37350254 Free PMC article.
-
A qualitative assessment of the diagnosis and management of ventilator-associated pneumonia among critical care clinicians exploring opportunities for diagnostic stewardship.Infect Control Hosp Epidemiol. 2022 Mar;43(3):284-290. doi: 10.1017/ice.2021.130. Epub 2021 Apr 16. Infect Control Hosp Epidemiol. 2022. PMID: 33858548
-
The efficiency of routine endotracheal aspirate cultures compared to bronchoalveolar lavage cultures in ventilator-associated pneumonia diagnosis.Niger J Clin Pract. 2016 Jan-Feb;19(1):46-51. doi: 10.4103/1119-3077.164327. Niger J Clin Pract. 2016. PMID: 26755218
-
Diagnosis of ventilator-associated pneumonia: controversies and working toward a gold standard.Curr Opin Infect Dis. 2013 Apr;26(2):140-50. doi: 10.1097/QCO.0b013e32835ebbd0. Curr Opin Infect Dis. 2013. PMID: 23411419 Review.
-
Ventilator-associated tracheobronchitis and pneumonia: thinking outside the box.Clin Infect Dis. 2010 Aug 1;51 Suppl 1:S59-66. doi: 10.1086/653051. Clin Infect Dis. 2010. PMID: 20597674 Review.
Cited by
-
The Evolving Landscape of Discrete Choice Experiments in Health Economics: A Systematic Review.Pharmacoeconomics. 2025 Aug;43(8):879-936. doi: 10.1007/s40273-025-01495-y. Epub 2025 May 21. Pharmacoeconomics. 2025. PMID: 40397369 Free PMC article.
-
Improving Antibiotic Use for Ventilator-Associated Pneumonia Through Diagnostic Stewardship: A Proof-of-Concept Mixed Methods Study.Open Forum Infect Dis. 2024 Sep 4;11(9):ofae500. doi: 10.1093/ofid/ofae500. eCollection 2024 Sep. Open Forum Infect Dis. 2024. PMID: 39319091 Free PMC article.
-
A qualitative investigation of paediatric intensive care staff attitudes towards the diagnosis of lower respiratory tract infection in the molecular diagnostics era.Intensive Care Med Paediatr Neonatal. 2023;1(1):10. doi: 10.1007/s44253-023-00008-z. Epub 2023 Jul 7. Intensive Care Med Paediatr Neonatal. 2023. PMID: 37425493 Free PMC article.
-
Potential role of report nudging on diagnosis and treatment of ventilator-associated pneumonia: a quantitative survey.Antimicrob Steward Healthc Epidemiol. 2025 Feb 17;5(1):e55. doi: 10.1017/ash.2025.43. eCollection 2025. Antimicrob Steward Healthc Epidemiol. 2025. PMID: 40026756 Free PMC article.
References
-
- Ferrer M, Torres A. Epidemiology of ICU-acquired pneumonia. Curr Opin Crit Care 2018;24:325–331. - PubMed
-
- Pneumonia (ventilator-associated [VAP] and non–ventilator-associated pneumonia [PNEU]) event table of contents. Centers for Disease Control and Prevention website. https//www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf. Published 2013. Accessed January 27, 2021.
-
- Nussenblatt V, Avdic E, Berenholtz S, et al. Ventilator-associated pneumonia: overdiagnosis and treatment are common in medical and surgical intensive care units. Infect Control Hosp Epidemiol 2014;35(3): 278–284. - PubMed
-
- Quick JA, Breite MD, Barnes SL. Inadequacy of algorithmic ventilator-associated pneumonia diagnosis in acute care surgery. Am Surg 2018;84:300–304. - PubMed
LinkOut - more resources
Full Text Sources