

Clinical burden of recurrent Clostridioides difficile infection in the medicare population: A real-world claims analysis
- PMID: 36483433
- PMCID: PMC9726521
- DOI: 10.1017/ash.2022.2
Clinical burden of recurrent Clostridioides difficile infection in the medicare population: A real-world claims analysis
Abstract
Objective: To describe 12-month outcomes for beneficiaries in the 100% Medicare Fee-for-Service (FFS) population with primary and recurrent Clostridioides difficile infection (CDI).
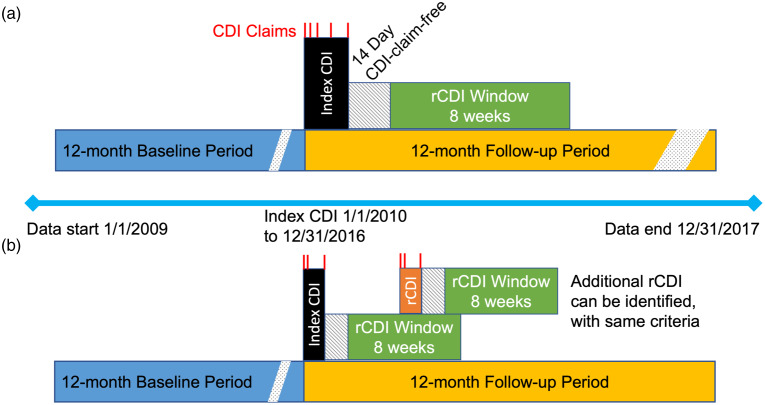
Design: A retrospective, descriptive, cohort study of CDI claims from the 100% Medicare FFS population, with a first CDI diagnosis between January 1, 2010, and December 31, 2016.
Setting: Any US-based provider that submitted inpatient or outpatient CDI diagnosis claims to Medicare FFS.
Patients: The study included patients aged ≥65 years with continuous enrollment in Medicare Parts A, B, and D during 12 months before and 12 months after the index period.
Methods: The number of CDI and recurrent (rCDI) episodes, healthcare resource utilization, treatments, complications, and procedures were calculated for pre-index and follow-up periods. The data were stratified by number of rCDI episodes (ie, no rCDI, 1 rCDI, 2 rCDI, and ≥3 rCDI).
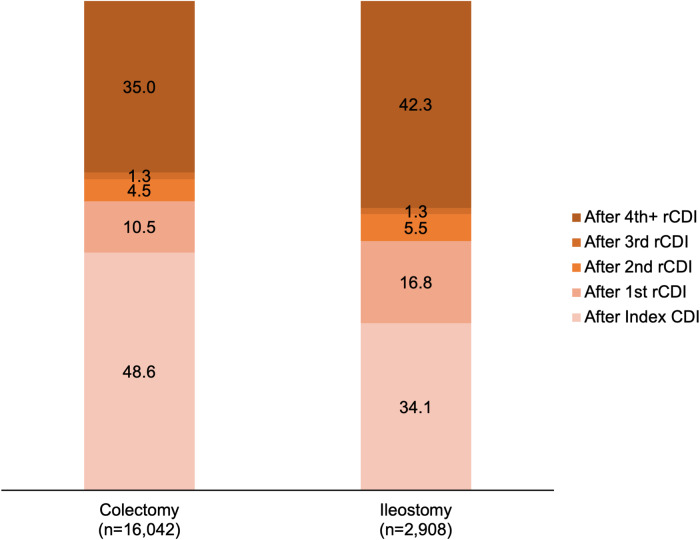
Results: Of 268,762 patients with an index CDI, 34.7% had at least 1 recurrence. Of those who had 1 recurrence, 59.1% had a second recurrence and of those who had 2 recurrences, 58.4% had ≥3 recurrences. Incident psychiatric conditions occurred in 11.3%-18.2% of each rCDI cohort; 6.0% of patients with rCDI underwent subtotal colectomy, and 1.1% of patients underwent diverting loop ileostomy. After each CDI episode, ∼1 in 5 patients had a documented sepsis event. Over the 12-month follow-up, 30% of patients experienced sepsis, and sepsis occurred in 27.0% of the cohort with no rCDI, compared to 35.5% of patients in the rCDI cohorts.
Conclusions: Elderly patients with CDI and rCDI experienced a significant clinical burden and complications.
© The Author(s) 2022.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources