

Percutaneous Thermal Ablation for Managing Small Renal Metastatic Tumors
- PMID: 36483663
- PMCID: PMC9719821
- DOI: 10.22575/interventionalradiology.2021-0032
Percutaneous Thermal Ablation for Managing Small Renal Metastatic Tumors
Abstract
Purpose: To retrospectively evaluate the treatment outcomes of thermal ablation for renal metastatic tumors.
Materials and methods: Thirteen consecutive patients with small renal metastatic tumors (≤3 cm), who underwent thermal ablation between 2009 and 2020, were included in this study. Eight patients had extra-renal tumors during renal ablation. The primary tumors were adenoid cystic carcinoma in four patients, lung cancer in three, hemangiopericytoma in three, leiomyosarcoma in two, and thyroid cancer in one. The therapeutic effects, safety, survival rate, prognostic factor, and renal function were evaluated.
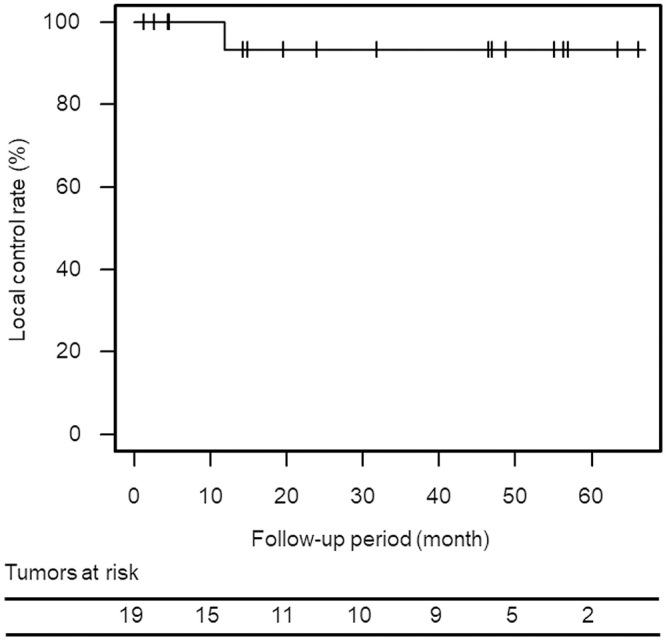
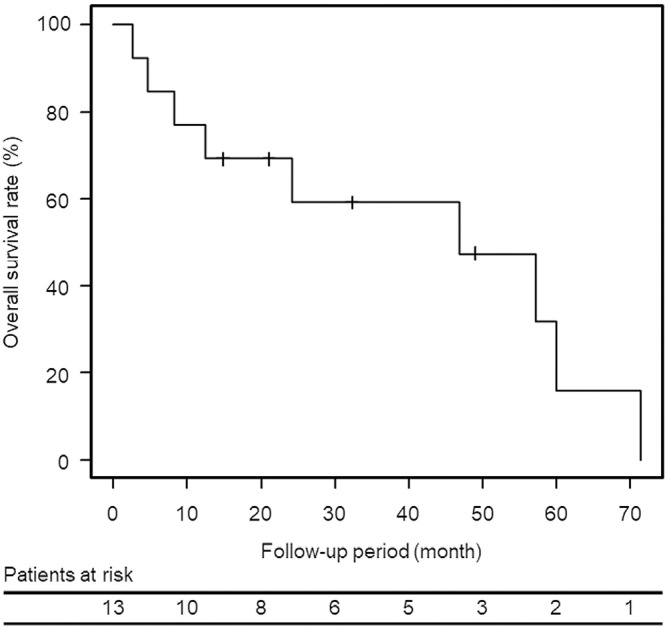
Results: We performed 18 ablation sessions (cryoablation, n = 13; radiofrequency ablation, n = 5) on 19 renal metastases with a mean diameter of 1.7 cm, which resulted in a primary technique efficacy rate of 100% without procedure-related deaths or major complications. Renal function significantly declined 6 months after ablation (P = 0.0039). During the mean follow-up period of 31.2 ± 22.4 months (range, 2.7-71.4 months), one patient had local tumor progression at 11.9 months following radiofrequency ablation. The overall survival rates at 1 and 3 years after ablation were 76.9% (95% confidence interval [CI], 54.0%-99.8%) and 59.3% (95% CI, 31.3%-87.3%), respectively. Tumor size ≥ 2 cm (P = 0.02) and metastasis from non-small cell lung cancer (P = 0.001) were significant worse prognostic factors in univariate analysis, and metastasis from non-small cell lung cancer (P = 0.01) was significant in multivariate analysis.
Conclusions: Percutaneous thermal ablation for small renal metastases is safe and feasible and can control local tumors.
Keywords: cryoablation; radiofrequency ablation; renal metastasis.
© 2022 Japanese Society of Interventional Radiology.
Conflict of interest statement
One of the authors (H.S.) has received research grants from DAIICHI SANKYO COMPANY, LIMITED, Fuji Pharma Co., Ltd., FUJIFILM RI Pharma Co., Ltd., and Eisai Co., Ltd. All other authors declare that there are no relevant conflicts of interest. This study was not supported by any funding.
Figures


Similar articles
-
Role of Repeated Radiofrequency Ablation for Patients with Lung Metastases of Head and Neck Adenoid Cystic Carcinoma: Long-term Single-center Study in 16 Patients with 289 Tumors.Interv Radiol (Higashimatsuyama). 2025 Feb 7;10:e20240015. doi: 10.22575/interventionalradiology.2024-0015. eCollection 2025 Mar 28. Interv Radiol (Higashimatsuyama). 2025. PMID: 40384900 Free PMC article.
-
Comparison of Percutaneous Image-Guided Microwave Ablation and Cryoablation for Sarcoma Lung Metastases: A 10-Year Experience.AJR Am J Roentgenol. 2022 Mar;218(3):494-504. doi: 10.2214/AJR.21.26551. Epub 2021 Oct 6. AJR Am J Roentgenol. 2022. PMID: 34612679
-
Percutaneous Ablation of T1 Renal Masses: Comparative Local Control and Complications after Radiofrequency and Cryoablation.Diagnostics (Basel). 2023 Sep 26;13(19):3059. doi: 10.3390/diagnostics13193059. Diagnostics (Basel). 2023. PMID: 37835802 Free PMC article.
-
Percutaneous ablation of renal masses measuring 3.0 cm and smaller: comparative local control and complications after radiofrequency ablation and cryoablation.AJR Am J Roentgenol. 2013 Feb;200(2):461-6. doi: 10.2214/AJR.12.8618. AJR Am J Roentgenol. 2013. PMID: 23345372
-
Percutaneous cryoablation of hepatic tumors: long-term experience of a large U.S. series.Abdom Radiol (NY). 2016 Apr;41(4):767-80. doi: 10.1007/s00261-016-0687-x. Abdom Radiol (NY). 2016. PMID: 26960728 Review.
References
-
- Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma. Analysis of 1000 autopsied cases. Cancer. 1950; 3: 74-85. - PubMed
-
- Bracken RB, Chica G, Johnson DE, Luna M. Secondary renal neoplasms: an autopsy study. South Med J. 1979; 72: 806-807. - PubMed
-
- Choyke PL, White EM, Zeman RK, Jaffe MH, Clark LR. Renal metastases: clinicopathologic and radiologic correlation. Radiology. 1987; 162: 359-363. - PubMed
-
- Pagani JJ. Solid renal mass in the cancer patient: second primary renal cell carcinoma versus renal metastasis. J Comput Assist Tomogr. 1983; 7: 444-448. - PubMed