

Nanoscopy and an extended lateral approach can improve the management of latero-central segments in tibial plateau fractures: a cadaveric study
- PMID: 36484798
- PMCID: PMC10229462
- DOI: 10.1007/s00068-022-02188-3
Nanoscopy and an extended lateral approach can improve the management of latero-central segments in tibial plateau fractures: a cadaveric study
Abstract
Introduction: The objective of this investigation was to compare different techniques to improve visualization and reduction in tibial plateau fractures involving the central lateral segments.
Methods: Matched pairs of pre-fractured cadaveric tibial plateau fractures that include the central lateral segments were treated by either an anterolateral approach (supine) or PL approach (prone). Reduction was stepwise extended by additional fracturoscopy (FS), nanoscopy (NS) and lastly by epicondyle osteotomy (ECO). Reduction was analyzed by 3D scan and visualization of the lateral plateau was quantified.
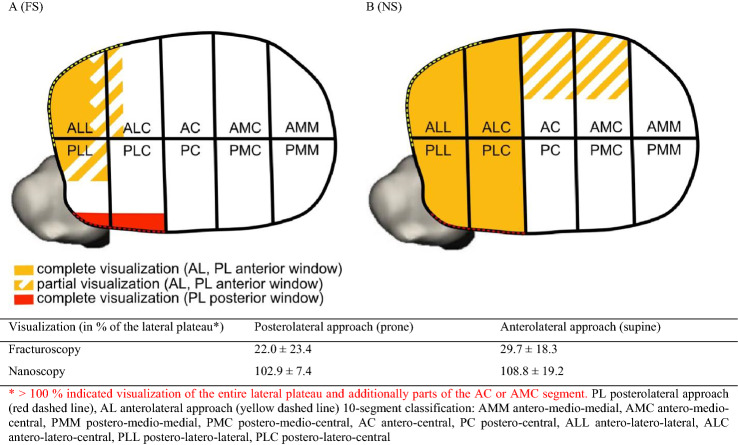
Results: Ten specimens (3 pairs 41B3.1, 2 pairs 41C3.3) were analyzed. Fracture steps involving the antero-latero-central (ALC) segment were insufficiently reduced after fluoroscopy using both approaches (AL 2.2 ± 1.2 mm vs PL 2.2 ± 1.0 mm, p 0.95). Additional NS and ECO achieved optimized fracture reduction in the ALC segment (NS AL 1.6 ± 1.3 mm vs PL 0.8 ± 0.9 mm, p 0.32). NS provided visualization of the entire lateral plateau (PL 102.9% ± 7.4, AL 108.8 ± 19.2%), while fracturoscopy only allowed visualization of the ALL segment and partially of PLL and ALC segments (PL 22.0 ± 23.4%, AL 29.7 ± 18.3%).
Conclusion: Optimized reduction of tibial head fractures with involvement of latero-central segments requires additional video-assisted reduction or extended approaches. Nanoscopy helps visualizing of the entire lateral plateau, when compared to fracturoscopy and may become a valuable reduction aid.
Keywords: Fracture; Nanoscope; Posterolateral approach; Prone; Supine; Tibia.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that this study was financially supported by Arthrex Inc. and Siemens. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results. PB was recipient of a fellowship of the German Knee Society sponsored by Arthrex Inc.
Figures

Similar articles
-
Lateral epicondyle osteotomy results in improved radiologic and functional outcomes in severe lateral tibial plateau fractures: a retrospective cohort study.J Orthop Surg Res. 2025 Apr 10;20(1):363. doi: 10.1186/s13018-025-05775-3. J Orthop Surg Res. 2025. PMID: 40211388 Free PMC article.
-
Anterolateral versus modified posterolateral approach for tibial plateau fractures with involvement of the posterior column: a cadaveric study.Eur J Trauma Emerg Surg. 2023 Feb;49(1):201-207. doi: 10.1007/s00068-022-02113-8. Epub 2022 Sep 28. Eur J Trauma Emerg Surg. 2023. PMID: 36171336 Free PMC article.
-
Clinical and radiological outcome of extended lateral approach via epicondyle osteotomy in complex lateral tibia plateau fractures involving the central and postero-lateral segments.Injury. 2024 Dec;55(12):111876. doi: 10.1016/j.injury.2024.111876. Epub 2024 Sep 27. Injury. 2024. PMID: 39423668
-
The concept of direct approach to lateral tibial plateau fractures and stepwise extension as needed.Eur J Trauma Emerg Surg. 2020 Dec;46(6):1211-1219. doi: 10.1007/s00068-020-01422-0. Epub 2020 Jun 30. Eur J Trauma Emerg Surg. 2020. PMID: 32607776 Free PMC article. Review.
-
[Osteosynthesis of bicondylar tibial plateau fracture in a prone position : Video article].Unfallchirurg. 2018 Dec;121(12):1004-1010. doi: 10.1007/s00113-018-0574-8. Unfallchirurg. 2018. PMID: 30402690 Review. German.
Cited by
-
Lack of standardisation in the management of complex tibial plateau fractures: a multicentre experience.Eur J Trauma Emerg Surg. 2024 Dec;50(6):2937-2945. doi: 10.1007/s00068-024-02616-6. Epub 2024 Aug 2. Eur J Trauma Emerg Surg. 2024. PMID: 39095621 Free PMC article.
-
Lateral epicondyle osteotomy results in improved radiologic and functional outcomes in severe lateral tibial plateau fractures: a retrospective cohort study.J Orthop Surg Res. 2025 Apr 10;20(1):363. doi: 10.1186/s13018-025-05775-3. J Orthop Surg Res. 2025. PMID: 40211388 Free PMC article.
-
Location of lateral tibial plateau fractures relative to the posterolateral complex predicts the need for extension of lateral approaches: A retrospective observational study.Eur J Trauma Emerg Surg. 2025 Jul 21;51(1):257. doi: 10.1007/s00068-025-02933-4. Eur J Trauma Emerg Surg. 2025. PMID: 40691664 Free PMC article.
-
Comparison of different intraoperative reduction monitoring methods in a cadaveric intraarticular calcaneal fracture model: 3D scan vs arthroscopy vs nanoscopy.Eur J Trauma Emerg Surg. 2023 Dec;49(6):2561-2567. doi: 10.1007/s00068-023-02330-9. Epub 2023 Aug 8. Eur J Trauma Emerg Surg. 2023. PMID: 37552339
-
Tibial plateau fractures are associated with ligamentous and meniscal injuries. Preoperative evaluation of magnetic resonance imaging influences surgical treatment.Eur J Trauma Emerg Surg. 2024 Oct;50(5):2367-2374. doi: 10.1007/s00068-024-02581-0. Epub 2024 Jun 26. Eur J Trauma Emerg Surg. 2024. PMID: 38926170 Free PMC article.
References
-
- Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, Prokuski L, Sirkin MS, Ziran B, Henley B, et al. Fracture and dislocation classification compendium—2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 2007;21:S1–133. doi: 10.1097/00005131-200711101-00001. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
