

Laparoscopic resection of an intra-abdominal esophageal duplication cyst in the ileum: a case report
- PMID: 36484876
- PMCID: PMC9733750
- DOI: 10.1186/s40792-022-01576-6
Laparoscopic resection of an intra-abdominal esophageal duplication cyst in the ileum: a case report
Abstract
Background: Esophageal duplication cyst (EDC) is a type of gastrointestinal duplication cyst that involves congenital malformations of the gastrointestinal tract. EDCs are frequently found in the mediastinum and thoracoabdominal region, but rarely occur in the abdominal cavity. However, intra-abdominal EDCs are frequently found in the upper abdomen near the abdominal esophagus. Here, we report, for the first time, a case of intra-abdominal EDC that occurred in the ileum.
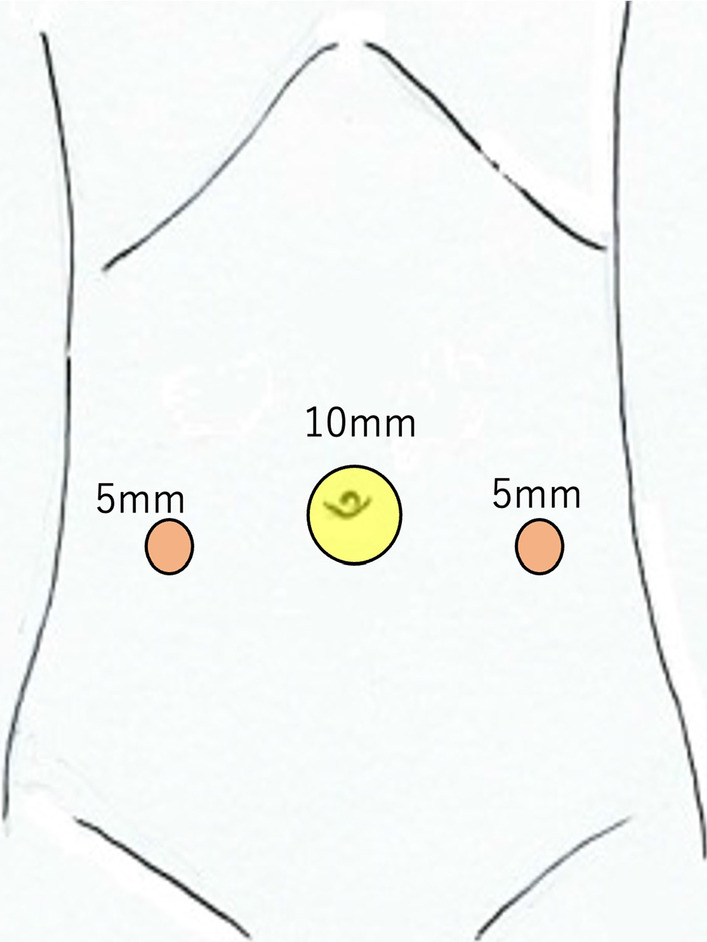
Case presentation: A 14-year-old female patient presented to our hospital with complaints of epigastric pain and vomiting. Abdominal computed tomography (CT) revealed a cystic tumor in the pelvis, suspected of ovarian origin. She was admitted to our gynecology department and underwent emergency surgery. The laparoscopic examination revealed that both ovaries were intact and that a primary tumor had developed from the ileal mesentery. Since the patient's condition was not urgent at the time of the gynecological surgery, the procedure was completed by only performing exploratory laparotomy; the patient was admitted to our department after the surgery. Pelvic magnetic resonance imaging performed on the next day revealed a cystic mass measuring 90 × 65 mm with a smooth margin and homogeneous signal intensity, arising posterior to the uterus. The mass was suspected as an intestinal duplication cyst. On another day, after the examinations were completed, we resected the portion of the small intestine containing the tumor by laparoscopy. The patient had a successful postoperative course and was discharged on the 5th postoperative day. Histological examination showed that the cyst was lined by stratified squamous epithelium, contained esophageal glands, and had a two-layer muscularis propria. Therefore, a diagnosis of intra-abdominal EDC was performed.
Conclusions: An intra-abdominal EDC cyst is relatively rare; this is the first case reported at the distal ileum.
Keywords: Ileum; Intra-abdominal esophageal duplication cyst; Laparoscopic surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures




References
LinkOut - more resources
Full Text Sources
