

Thrombocytopenia in pregnancy
- PMID: 36485110
- PMCID: PMC9820693
- DOI: 10.1182/hematology.2022000375
Thrombocytopenia in pregnancy
Abstract
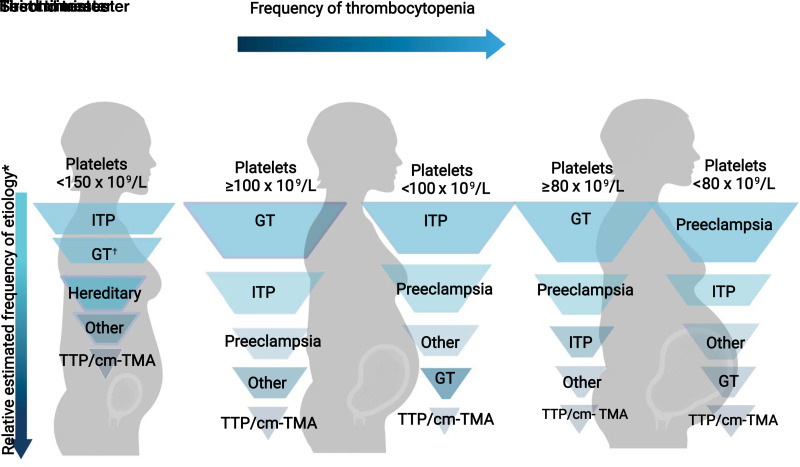
Hematologists are often consulted for thrombocytopenia in pregnancy, especially when there is a concern for a non-pregnancy-specific etiology or an insufficient platelet count for the hemostatic challenges of delivery. The severity of thrombocytopenia and trimester of onset can help guide the differential diagnosis. Hematologists need to be aware of the typical signs of preeclampsia with severe features and other hypertensive disorders of pregnancy to help distinguish these conditions, which typically resolve with delivery, from other thrombotic microangiopathies (TMAs) (eg, thrombotic thrombocytopenic purpura or complement-mediated TMA). Patients with chronic thrombocytopenic conditions, such as immune thrombocytopenia, should receive counseling on the safety and efficacy of various medications during pregnancy. The management of pregnant patients with chronic immune thrombocytopenia who are refractory to first-line treatments is an area that warrants further research. This review uses a case-based approach to discuss recent updates in diagnosing and managing thrombocytopenia in pregnancy.
Copyright © 2022 by The American Society of Hematology.
Conflict of interest statement
Allyson M. Pishko has received research funding on behalf of her institution from an educational grant from Sanofi Genzyme.
Ariela L. Marshall: no competing financial interests to declare.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources