

Treatment of Richter's syndrome
- PMID: 36485138
- PMCID: PMC9820569
- DOI: 10.1182/hematology.2022000345
Treatment of Richter's syndrome
Abstract
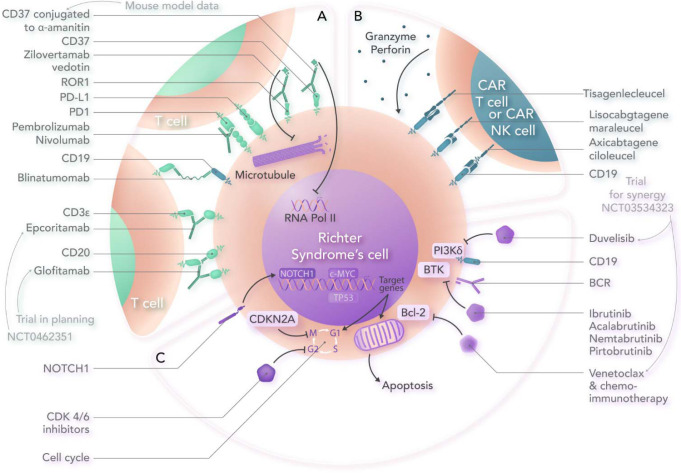
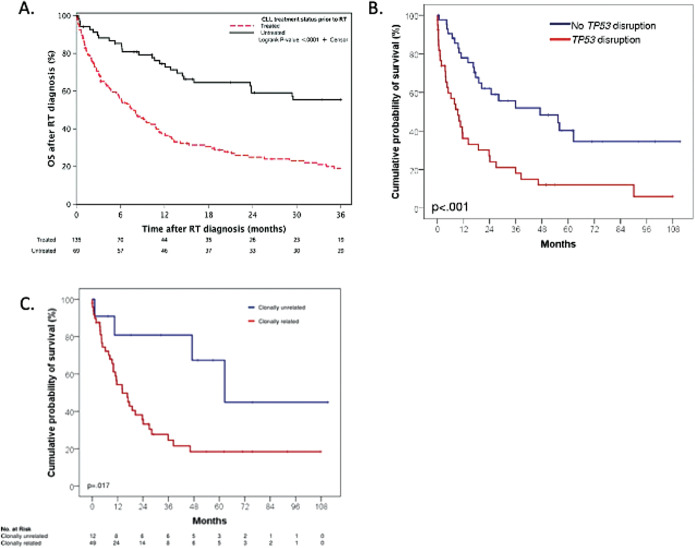
Richter's syndrome (RS) is an aggressive histologic transformation of chronic lymphocytic leukemia (CLL), most commonly to diffuse large B-cell lymphoma (DLBCL). Outcomes are generally poor, with complete remission (CR) rates of only about 20% and less than 20% long-term survival with chemoimmunotherapy (CIT). RS is biologically heterogeneous, and in 80% of patients with CLL who develop DLBCL, the disease is clonally related to the CLL. Clonally unrelated cases are genetically and immunologically distinct from clonally related DLBCL-RS, have more favorable responses to CIT, and are best treated as de novo DLBCL. Relatively favorable outcomes with CIT are also seen in patients who have never previously received treatment for CLL and who lack TP53 mutation or deletion. For the remaining patients, treatment on a clinical trial is optimal. Fortunately, numerous agents are now in clinical development that show encouraging results. Here we review clinical data for some of the most promising approaches. DLBCL-RS tumor cells frequently express programmed cell death 1 protein (PD-1), and several studies have demonstrated activity for PD-1 inhibitors, especially in combination with ibrutinib. The BCL2 inhibitor venetoclax in combination with R-EPOCH CIT achieved CR in 50% of patients, and a study of venetoclax-R-CHOP is ongoing. The noncovalent Bruton's tyrosine kinase inhibitor pirtobrutinib has achieved responses in approximately two-thirds of heavily pretreated patients and, given its favorable toxicity profile, appears ideally suited to combining with other active agents. Finally, we review available data for bispecific antibodies, antibody-drug conjugates, and chimeric antigen receptor T-cell therapy, which, after revolutionizing the treatment of DLBCL, are now being evaluated in RS.
Copyright © 2022 by The American Society of Hematology.
Conflict of interest statement
Philip A. Thompson: research funding: Adaptive Biotechnologies, Genentech, AbbVie, Pharmacyclics, Amgen, Lilly; advisory board: Adaptive Biotechnologies, Janssen, Pharmacyclics, AstraZeneca, Beigene, AbbVie, Genentech, Lilly; lecturer: Janssen Australia.
Tanya Siddiqi: speaker: Astra Zeneca, Bristol Myers Squibb, BeiGene; advisory board: Astra Zeneca, BeiGene, Bristol Myers Squibb, Celgene, AbbVie, Pharmacyclics, Gilead; honoraria: Dava Oncology, ResearchToPractice.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous