

How I prevent viral reactivation in high-risk patients
- PMID: 36493341
- PMCID: PMC10163320
- DOI: 10.1182/blood.2021014676
How I prevent viral reactivation in high-risk patients
Abstract
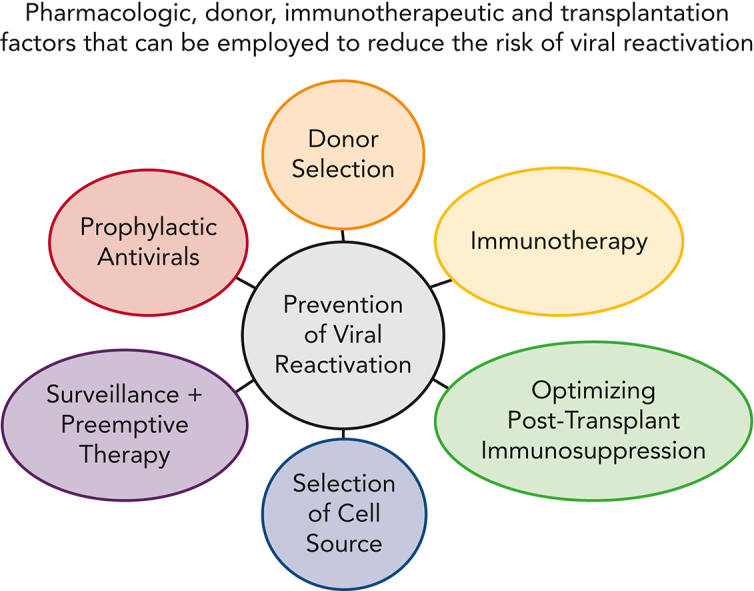
Preventing viral infections at an early stage is a key strategy for successfully improving transplant outcomes. Preemptive therapy and prophylaxis with antiviral agents have been successfully used to prevent clinically significant viral infections in hematopoietic cell transplant recipients. Major progress has been made over the past decades in preventing viral infections through a better understanding of the biology and risk factors, as well as the introduction of novel antiviral agents and advances in immunotherapy. High-quality evidence exists for the effective prevention of herpes simplex virus, varicella-zoster virus, and cytomegalovirus infection and disease. Few data are available on the effective prevention of human herpesvirus 6, Epstein-Barr virus, adenovirus, and BK virus infections. To highlight the spectrum of clinical practice, here we review high-risk situations that we handle with a high degree of uniformity and cases that feature differences in approaches, reflecting distinct hematopoietic cell transplant practices, such as ex vivo T-cell depletion.
© 2023 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: S.S.D. has received research support (funds paid to institution) from Merck, Ansun Biopharma, AlloVir, Gilead, Geovax, Amplyx, and Karius; consulting/advisory board fees from Merck, AlloVir, and Aseptiscope; and speakers’ bureau fees from Takeda, Merck, and Astellas, all outside the submitted work. G.A.P. has received research support (funds paid to institution) from Merck and Shire Pharmaceutical (now known as Takeda) and consulting/other fees from AlloVir, Amplyx, Cidara, Merck & Co, Octapharma, SLC Behring, Takeda, SymBio, and Vera, all outside the submitted work. M.B. has received research support (funds paid to institution) from Astellas, Gilead Sciences, Shire Pharmaceutical (now known as Takeda), and Merck & Co Inc; consulting fees from Merck & Co Inc, AlloVir, and SymBio; and consulting fees and the rights to acquire equity from EvrysBio and Helocyte, all outside of the submitted work.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
