

Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial
- PMID: 36493792
- PMCID: PMC11200328
- DOI: 10.1016/S1470-2045(22)00694-5
Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial
Abstract
Background: Adjuvant abemaciclib plus endocrine therapy previously showed a significant improvement in invasive disease-free survival and distant relapse-free survival in hormone receptor-positive, human epidermal growth factor receptor 2 (HER2; also known as ERBB2)-negative, node-positive, high-risk, early breast cancer. Here, we report updated results from an interim analysis to assess overall survival as well as invasive disease-free survival and distant relapse-free survival with additional follow-up.
Methods: In monarchE, an open-label, randomised, phase 3 trial, adult patients (aged ≥18 years) who had hormone receptor-positive, HER2-negative, node-positive, early breast cancer at a high risk of recurrence with an Eastern Cooperative Oncology Group performance status of 0 or 1 were recruited from 603 sites including hospitals and academic and community centres in 38 countries. Patients were randomly assigned (1:1) by means of an interactive web-based response system (block size of 4), stratified by previous chemotherapy, menopausal status, and region, to receive standard-of-care endocrine therapy of physician's choice for up to 10 years with or without abemaciclib 150 mg orally twice a day for 2 years (treatment period). All therapies were administered in an open-label manner without masking. High-risk disease was defined as either four or more positive axillary lymph nodes, or between one and three positive axillary lymph nodes and either grade 3 disease or tumour size of 5 cm or larger (cohort 1). A smaller group of patients were enrolled with between one and three positive axillary lymph nodes and Ki-67 of at least 20% as an additional risk feature (cohort 2). This was a prespecified overall survival interim analysis planned to occur 2 years after the primary outcome analysis for invasive disease-free survival. Efficacy was assessed in the intention-to-treat population. Safety was assessed in all treated patients. The study is registered with ClinicalTrials.gov, NCT03155997, and is ongoing.
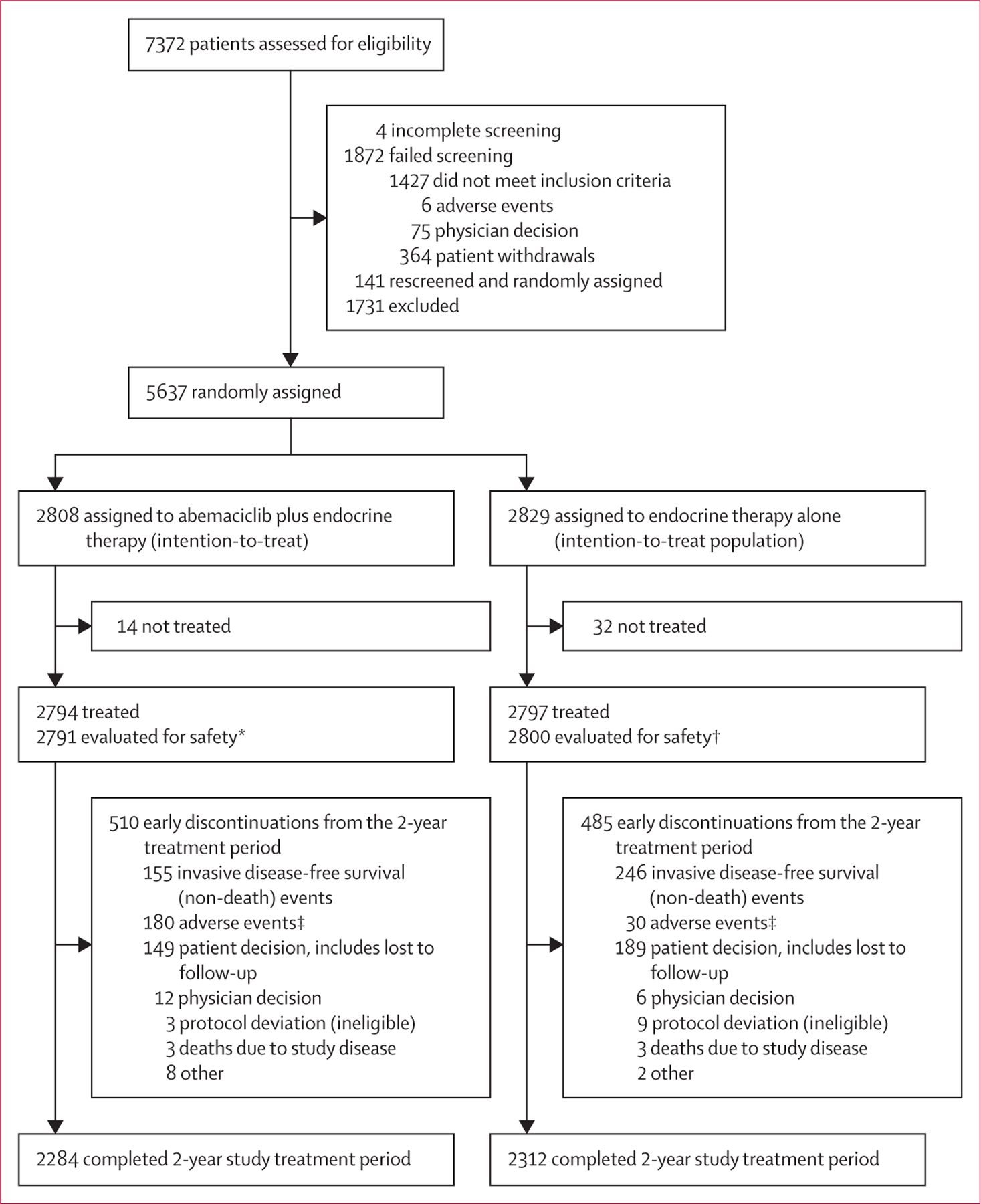
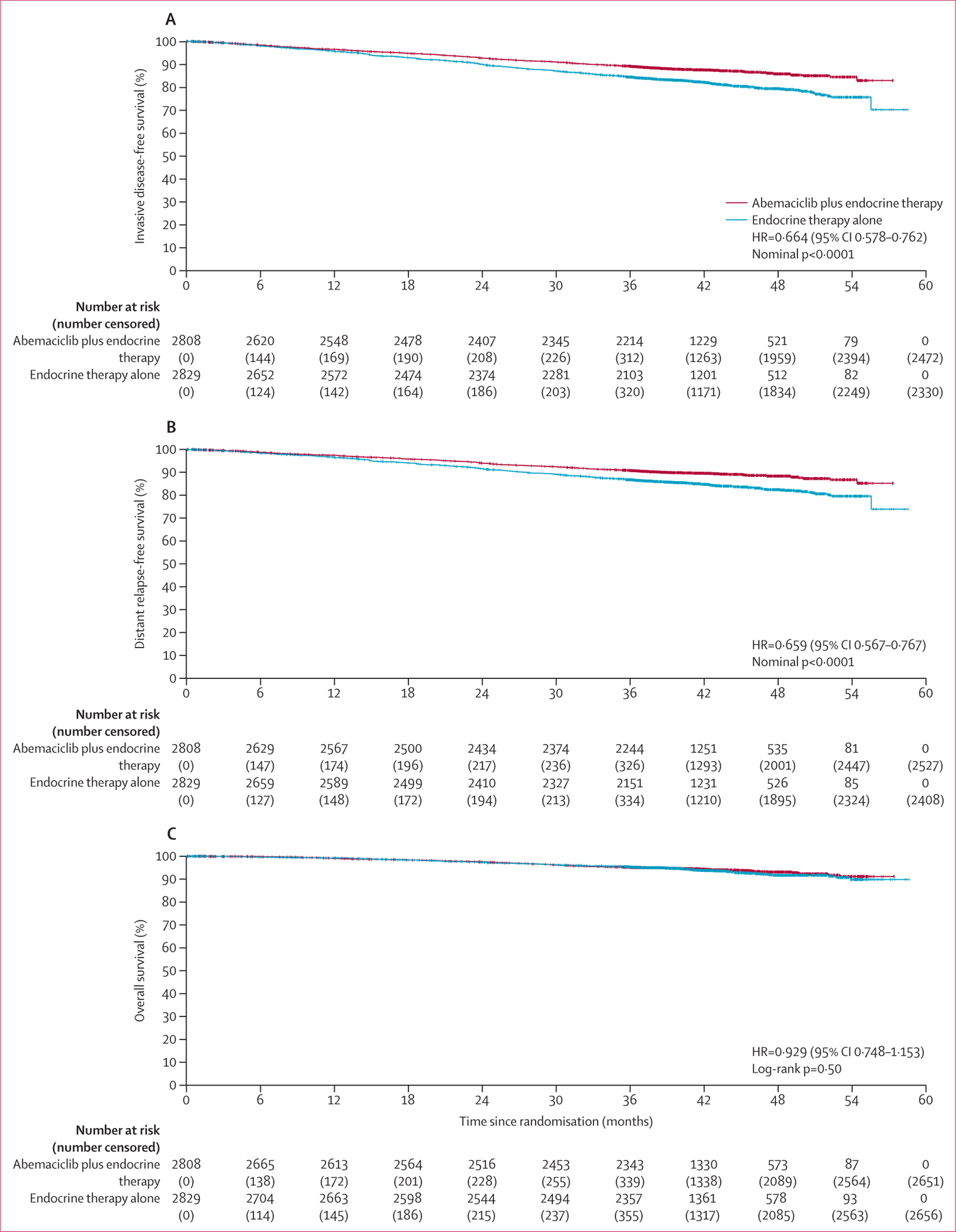
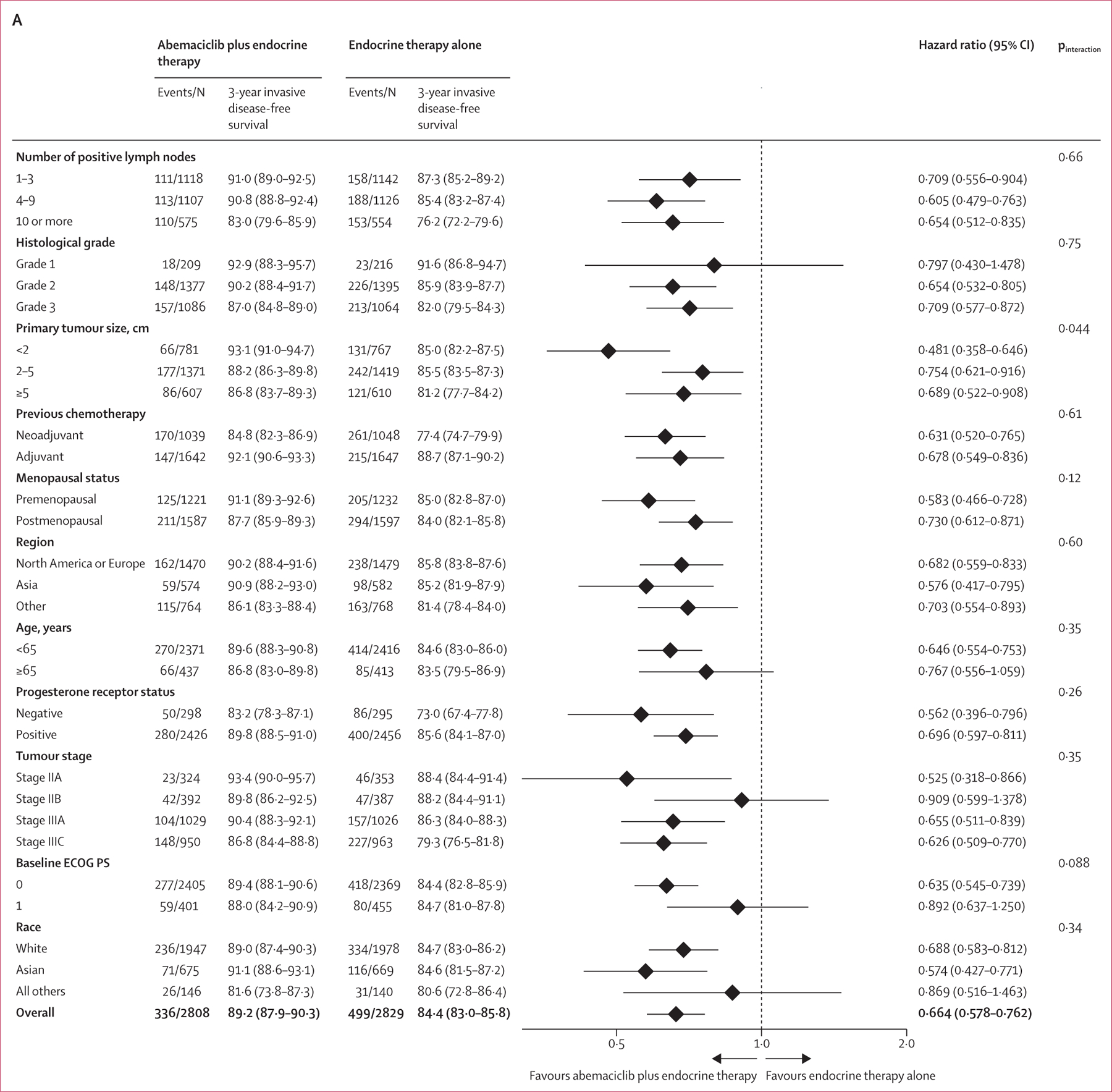
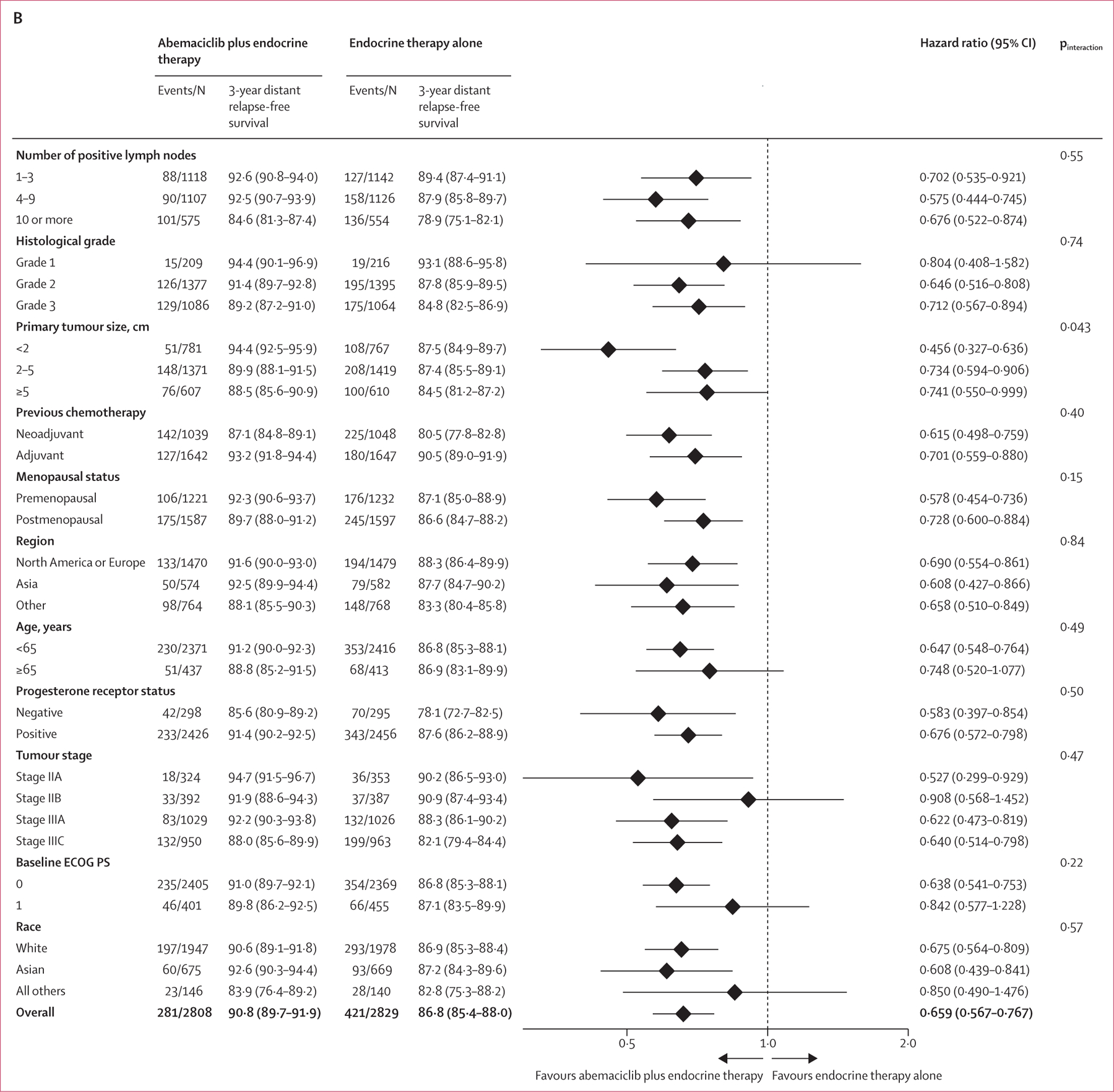
Findings: Between July 17, 2017, and Aug 12, 2019, 5637 patients were randomly assigned (5601 [99·4%] were women and 36 [0·6%] were men). 2808 were assigned to receive abemaciclib plus endocrine therapy and 2829 were assigned to receive endocrine therapy alone. At a median follow-up of 42 months (IQR 37-47), median invasive disease-free survival was not reached in either group and the invasive disease-free survival benefit previously reported was sustained: HR 0·664 (95% CI 0·578-0·762, nominal p<0·0001). At 4 years, the absolute difference in invasive disease-free survival between the groups was 6·4% (85·8% [95% CI 84·2-87·3] in the abemaciclib plus endocrine therapy group vs 79·4% [77·5-81·1] in the endocrine therapy alone group). 157 (5·6%) of 2808 patients in the abemaciclib plus endocrine therapy group died compared with 173 (6·1%) of 2829 patients in the endocrine therapy alone group (HR 0·929, 95% CI 0·748-1·153; p=0·50). The most common grade 3-4 adverse events were neutropenia (in 548 [19·6%] of 2791 patients receiving abemaciclib plus endocrine therapy vs 24 [0·9%] of 2800 patients in the endocrine therapy alone group), leukopenia (318 [11·4%] vs 11 [0·4%]), and diarrhoea (218 [7·8%] vs six [0·2%]). Serious adverse events occurred in 433 (15·5%) of 2791 patients receiving abemaciclib plus endocrine therapy versus 256 (9·1%) of 2800 receiving endocrine therapy. There were two treatment-related deaths in the abemaciclib plus endocrine therapy group (diarrhoea and pneumonitis) and none in the endocrine therapy alone group.
Interpretation: Adjuvant abemaciclib reduces the risk of recurrence. The benefit is sustained beyond the completion of treatment with an absolute increase at 4 years, further supporting the use of abemaciclib in patients with high-risk hormone receptor-positive, HER2-negative early breast cancer. Further follow-up is needed to establish whether overall survival can be improved with abemaciclib plus endocrine therapy in these patients.
Funding: Eli Lilly.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SRDJ reports grants or contracts from Pfizer, Puma Biotechnology, Eli Lilly, AstraZeneca, Novartis, and Roche–Genentech for research funding to institute for laboratory studies and clinical trials; consulting fees from Eli Lilly, AstraZeneca, Puma Biotechnology, Pfizer, Novartis, and Sanofi Genzyme for consulting or an advisory role; and payment or honoraria from Pfizer, Eisai, AstraZeneca, and Roche–Genentech for speaker's bureau. MT reports grants or contracts from Chugai, Takeda, Pfizer, Taiho, JBCRG, KBCRN, Eisai, Eli Lilly, Daiichi-Sankyo, AstraZeneca, Astellas, Shimadzu, Yakult, Nippon Kayaku, AFI technology, Luxonus, Shionogi, GL Science, and Sanwa Shurui for research grants to their department; payment or honoraria from Chugai, Takeda, Pfizer, Kyowa-Kirin, Taiho, Eisai, Daiichi-Sankyo, AstraZeneca, Eli Lilly, Merck Sharp and Dohme, Exact Science, Novartis, Shimadzu, Yakult, Nippon Kayaku, Devicore Medical Japan, and Sysmex for lecture honoraria or honoraria for lecture chair; participation on a data safety monitoring board or advisory board for Daiichi-Sankyo, Eli Lilly, Bristol Myers Squibb, Athenex Oncology, Bertis, Terumo, and Kansai Medical Net; and other financial or non-financial interest from British Journal of Cancer, Scientific Reports, Breast Cancer Research and Treatment, Cancer Science, Frontiers in Women's Cancer, Asian Journal of Surgery, and Asian Journal of Breast Surgery for his role as Associate Editor. JO'S reports consulting fees and payment or honoraria for lectures, presentations, speaker's bureaus, manuscript writing or educational events from from AbbVie, Agendia, Amgen Biotechnology, Aptitude Health, AstraZeneca, Athenex, Bayer, Bristol Myers Squibb, Carrick Therapeutics, Celgene Corporation, Daiichi Sankyo, Eisai, G1 Therapeutics, Genentech, Genzyme, Gilead Sciences, GRAIL, Halozyme Therapeutics, Heron Therapeutics, Immunomedics, Ipsen Biopharmaceuticals, Eli Lilly, Merck, Myriad, Nektar Therapeutics, Novartis, Ontada, Pfizer, Pharmacyclics, Pierre Fabre Pharmaceuticals, Puma Biotechnology, Prime Oncology, Roche, Samsung Bioepsis, Sandoz, Sanofi, Seagen, Syndax Pharmaceuticals, Taiho Oncology, Takeda, Theralink, and Synthon. MC reports personal payment support from Eli Lilly for the present article, advisory board, and speaker's bureau; payment or honoraria to institution from Novartis; support for attending meetings from Eli Lilly, Novartis, AstraZeneca, and Pfizer; and payment to institution from AstraZeneca, Novartis, Sanofi, Pfizer, Seagen, Gilead, Daiichi Sankyo for participation on a data safety monitoring board or advisory board. C-SH reports research grants to institution from Eli Lilly for the present article; research grants to institution or contracts from Daiichi Sankyo, AstraZeneca, EirGenix, Eli Lilly and Company, Merck Sharp and Dohme, OBI Pharma, Pfizer, Roche, and Novartis; payment or honoraria from Daiichi Sankyo, AstraZeneca, Pfizer, Novartis, Roche, and Eli Lilly for speaker's bureau; support for attending meetings or travel from Astra Zeneca, Pfizer, Roche, and Novartis; and participation on advisory boards from Daiichi Sankyo, AstraZeneca, Eli Lilly, Pfizer, Novartis, and Roche. JH reports institutional grants or contracts from Celgene, Novartis, Hexal, and Eli Lilly; consulting fees paid to self from Eli Lilly, Novartis, Roche, Pfizer, Hexal, AstraZeneca, Merck Sharp and Dohme, Celgene, AbbVie, and Daiichi-Sankyo; honoraria or payments to self for lectures, presentation, speaker's bureaus, manuscript writing, or educational events from Eli Lilly, Novartis, Roche, Pfizer, AstraZeneca, Merck Sharp and Dohme, Celgene, Eisai, Abbvie, Seagen, and Gilead; and support for attending meetings or travel paid to self from Roche, Pfizer, Novartis, Celgene, Daiichi-Sankyo, and Gilead. SMT reports institutional funding for study, consulting work to personal (honorariums), and manuscript preparation from Eli Lilly; institutional grants or contracts from AstraZeneca, Merck, Mektar, Novartis, Pfizer, Genentech–Roche, Gilead, Exelixis, Bristol Myers Squibb, Eisai, Nanostring, Cyclacel, Sanofi, and Seagen; and honoraria payments to self for participation in advisory boards or consulting from AstraZeneca, Eli Lilly, Merck, Novartis, Pfizer, Genentech–Roche, Gilead, Bristol Myers Squibb, Eisai, Sanofi, Seagen, Daiichi-Sankyo, Athenex, OncoPep, Kyowa Kirin Pharma, CytomX, Certara, Mersana Therapeutics, Ellipses Pharma, 4D Pharma, OncoSec, Infinity Therapeutics, BeyondSpring Pharma, OncXerna, Zymeworks, Zentalis, ARC Therapeutics, Reveal Genomics, Blueprint Medicines, Myovant, Umoja Biopharma, and Menarini–Stemline. MPG reports institutional grants or contracts from Pfizer, Eli Lilly, and Sermonix; consulting fees to institution from Eagle Pharmaceuticals, Eli Lilly, Biovica, Novartis, Sermonix, Pfizer, and ARC Therapeutics; honoraria or payment to self for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from Research to Practice, Clinical Education Alliance, Medscape, Total Health Conferencing, Curio Science, and MJH Life Sciences; and support to institution from Eli Lilly, AstraZeneca, Novartis, Biotheranostics, Blueprint Medicines, Sanofi Genzyme, and ARC Therapeutics for participation on a data safety monitoring board or advisory board. HSR reports institutional research support from Pfizer, Novartis, Eli Lilly, Genentech–Roche, OBI, Merck, Gilead Sciences, Daiichi Sankyo, Seattle Genetics, Sermonix, AstraZeneca, and Astellas; travel support to academic meetings from Merck, AstraZeneca, and Gilead; and consulting or advisory support from Puma, NAPO, and Blueprint. ES reports support from Eli Lilly for the present article including investigator fees and medical writing; payment or honoraria for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from AstraZeneca, Cancérodigest, Curio, Science, Egis, Eli Lilly and Company, Exact Sciences, Gilead, high5md, Merck Sharp and Dohme, Novartis, Pfizer, and Pierre Fabre; support for attending meetings or travel from Egis, Gilead, Novartis, Pfizer, and Roche; participation on a data safety monitoring board or advisory board from AstraZeneca, Egis, Eli Lilly, Exact Sciences, Merck Sharp and Dohme, Novartis, and Pfizer; a leadership or fiduciary role from Stowarzyszenie Różowy Motyl as Chair (unpaid); stock or stock options from AstraZeneca, Eli Lilly, and Pfizer; receipt of equipment, materials, drugs, medical writing, gifts or other services from Astellas, AstraZeneca, and Eli Lilly; and other financial or non-financial interests from Amgen, AstraZeneca, Eli Lilly, Novartis, OBI Pharma, Pfizer, Roche, and Samsung for contracted research. LT reports support from Eli Lilly as the trial sponsor for the study; grants or contracts from Novartis for clinical research; consulting fees from Merck Sharp and Dohme, Eli Lilly, and Novartis for advisory board; payment or honoraria from Merck Sharp and Dohme, Eli Lilly, Pfizer, Daiichi Sankyo, Novartis, and AstraZeneca for medical education; and support for attending meetings or travel from Pfizer and AstraZeneca. LDM reports an institutional research grant from Eli Lilly, Novartis, Roche, Daiichi Sankyo, and Seagen; consulting fees paid to self from Eli Lilly; honoraria or payment to self from Roche, Novartis, Pfizer, Eli Lilly, AstraZeneca, Merck Sharp and Dohme, Seagen, Gilead, Pierre Fabre, Eisa, Exact Sciences, and Ipsen for lectures, presentations, speaker's bureaus, manuscript writing or educational events; support for attending meetings or travel from Roche, Pfizer, and Eisai; and fees paid to self for participation on a data safety monitoring board or advisory Board from Novartis, Roche, Eli Lilly, Pfizer, Daiichi-Sankyo, Exact Sciences, Gilead, Pierre Fabre, Eisai, AstraZeneca, and Agendia. CS reports research grants from Eli Lilly, and honoraria for lectures from Pfizer and Eli Lilly. RW, AS, MMu, BSA, VA are employees and stock shareholders of Eli Lilly. NH reports support for the present article (medical writing) from Eli Lilly; consulting fees from Gilead, Sandoz, and Seagen; payment or honoraria for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from Amgen, AsraZeneca, Daiichi-Sankyo, Gilead, Eli Lilly, Merck Sharp and Dohme, Novartis, Pierre-Fabre, Pfizer, Roche, and Seagen; participation on a data safety monitoring board or advisory board from Roche; and a leadership or fiduciary role with the West German Study Group and ESMO. MMa reports institutional grants from Roche, Novartis, and Puma; consulting fees paid to self from Roche, Eli Lilly, Pfizer, Daiichi-Sankyo, AstraZeneca, and Novartis; payment or honoraria to self for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from Roche, Eli Lilly, Astrazeneca, and Pfizer; support paid to self for attending meetings or travel from Daiichi-Sankyo and Roche; and support paid to self for participation on a data safety monitoring board or advisory board from Novartis. PR, PN, GGJ, and IC declare no competing interests.
Figures
Comment in
-
Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk, early breast cancer.Lancet Oncol. 2023 Mar;24(3):e103. doi: 10.1016/S1470-2045(23)00014-1. Lancet Oncol. 2023. PMID: 36858724 No abstract available.
-
Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk, early breast cancer - Authors' reply.Lancet Oncol. 2023 Mar;24(3):e104. doi: 10.1016/S1470-2045(23)00065-7. Lancet Oncol. 2023. PMID: 36858725 No abstract available.
-
The MonarchE trial: improving the clinical outcome in HR+ /HER2- early breast cancer: recent results and next steps.Cancer Commun (Lond). 2023 Aug;43(8):938-942. doi: 10.1002/cac2.12466. Epub 2023 Jul 18. Cancer Commun (Lond). 2023. PMID: 37462449 Free PMC article. No abstract available.
References
-
- Sheffield KM, Peachey JR, Method M, et al. A real-world US study of recurrence risks using combined clinicopathological features in HR-positive, HER2-negative early breast cancer. Future Oncol 2022; 18: 2667–82. - PubMed
-
- Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol 2021; 32: 1571–81. - PubMed
-
- Verzenio (abemaciclib) [package insert]. Indianapolis, IN: Eli Lilly, 2021.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
