

SARS-CoV-2 primary and breakthrough infections in patients with cancer: Implications for patient care
- PMID: 36494154
- PMCID: PMC9526006
- DOI: 10.1016/j.beha.2022.101384
SARS-CoV-2 primary and breakthrough infections in patients with cancer: Implications for patient care
Abstract
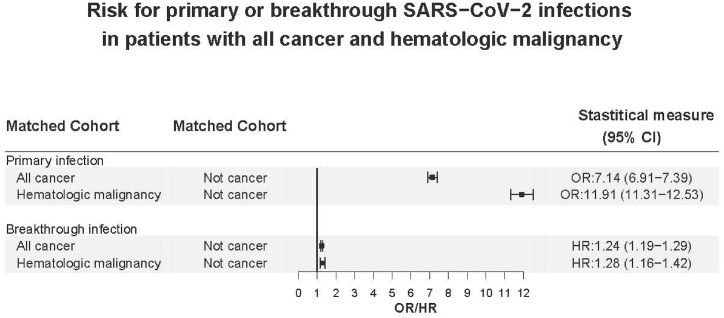
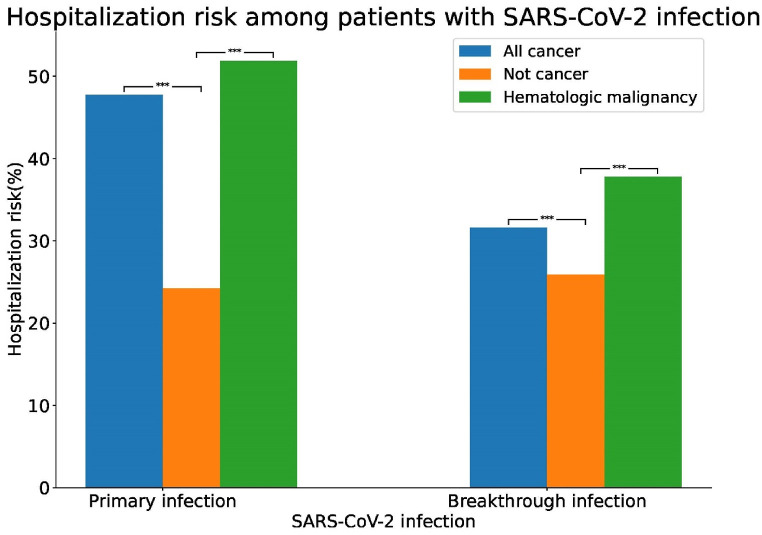
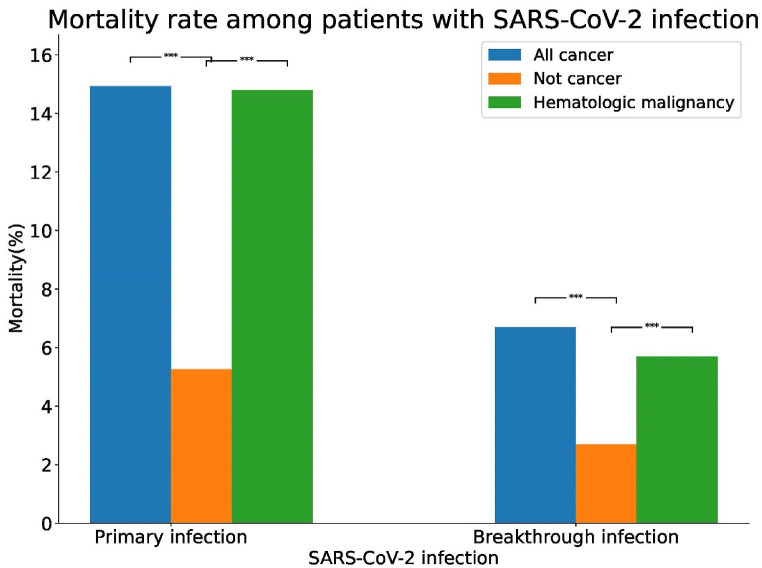
Initial reports of SARS-CoV-2 caused COVID-19 suggested that patients with malignant diseases were at increased risk for infection and its severe consequences. In order to provide early United States population-based assessments of SARS-CoV-2 primary infections in unvaccinated patients with hematologic malignancies or cancer, and SARS-CoV-2 breakthrough infections in vaccinated patients with hematologic malignancies or cancer, we conducted retrospective studies using two, unique nationwide electronic health records (EHR) databases. Using these massive databases to provide highly statistically significant data, our studies demonstrated that, compared to patients without malignancies, risk for COVID-19 was increased in patients with all cancers and with all hematologic malignancies. Risks varied with specific types of malignancy. Patients with hematologic malignancies or cancer were at greatest risk for COVID-19 during the first year after diagnosis. Risk for infection was increased for patients 65 years and older, compared to younger patients and among Black patients compared to white patients. When patients with hematologic malignancies or cancer were vaccinated against SARS-CoV-2, their risk for breakthrough infections was decreased relative to primary infections but remained elevated relative to vaccinated patients without malignancies. Compared to vaccinated patients without malignancies, vaccinated patients with hematologic malignancy or cancer showed increased risk for infection at earlier post vaccination time points. As with primary infections, risk for breakthrough infections was greatest in patients during their first year of hematologic malignancy or cancer. There were no signs of racial disparities among vaccinated patients with hematologic malignancies or cancer. These results provide the population basis to understand the significance of subsequent immunologic studies showing relative defective and delayed immunoresponsiveness to SARS-CoV-2 vaccines among patients with hematologic malignancies and cancers. These studies further provide the basis for recommendations regarding COVID-19 vaccination, vigilance and maintaining mitigation strategies in patients with hematologic malignancies and cancers.
Keywords: COVID-19; Cancer; Hematologic malignancies; SARS-CoV-2.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest All authors declare no conflict of interest.
Figures
References
-
- CDC Museum COVID-19 Timeline [Internet] U.S. Department of health & human services. https://www.cdc.gov/museum/timeline/covid19.html [cited 17 August 2022]. Available from:
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
