

SARS-CoV-2 Spike triggers barrier dysfunction and vascular leak via integrins and TGF-β signaling
- PMID: 36494335
- PMCID: PMC9734751
- DOI: 10.1038/s41467-022-34910-5
SARS-CoV-2 Spike triggers barrier dysfunction and vascular leak via integrins and TGF-β signaling
Abstract
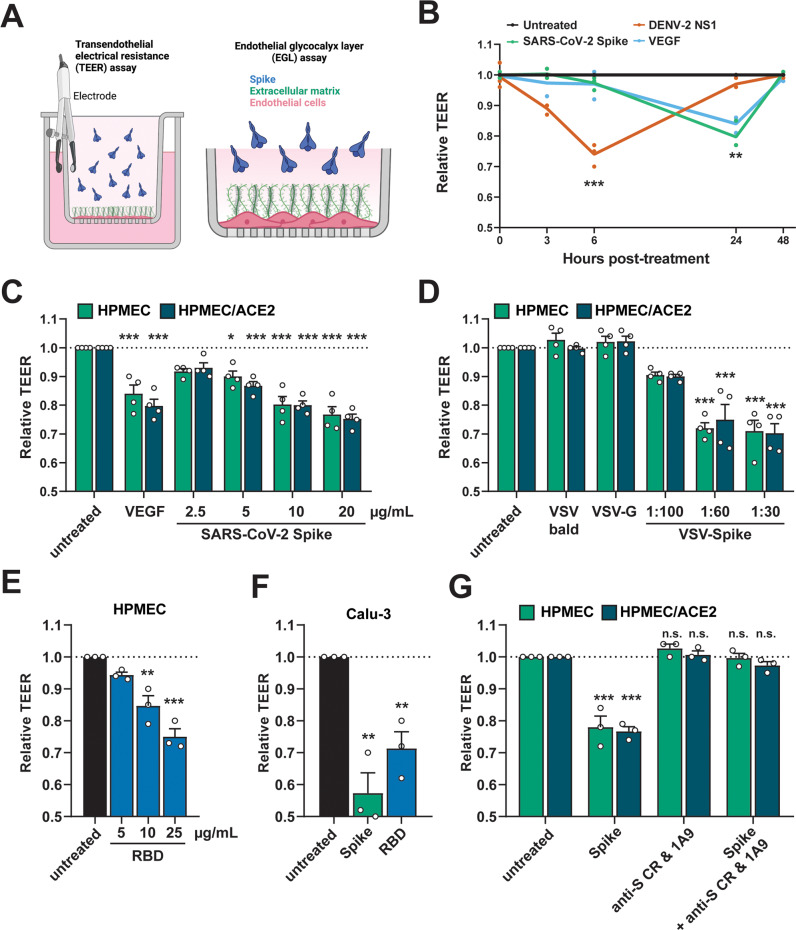
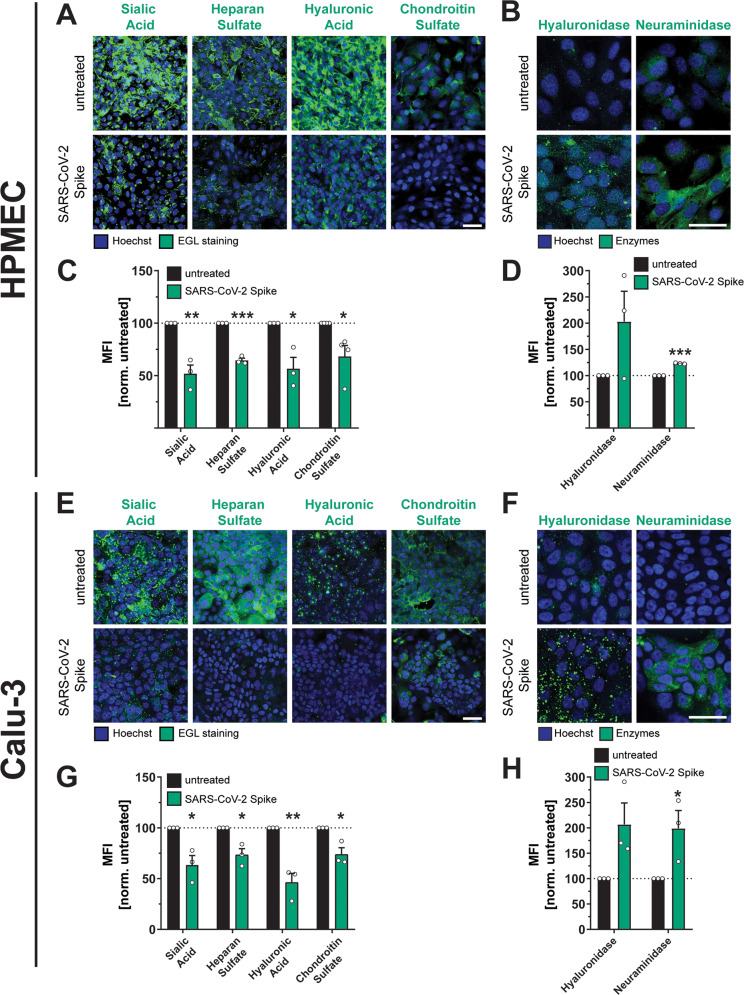
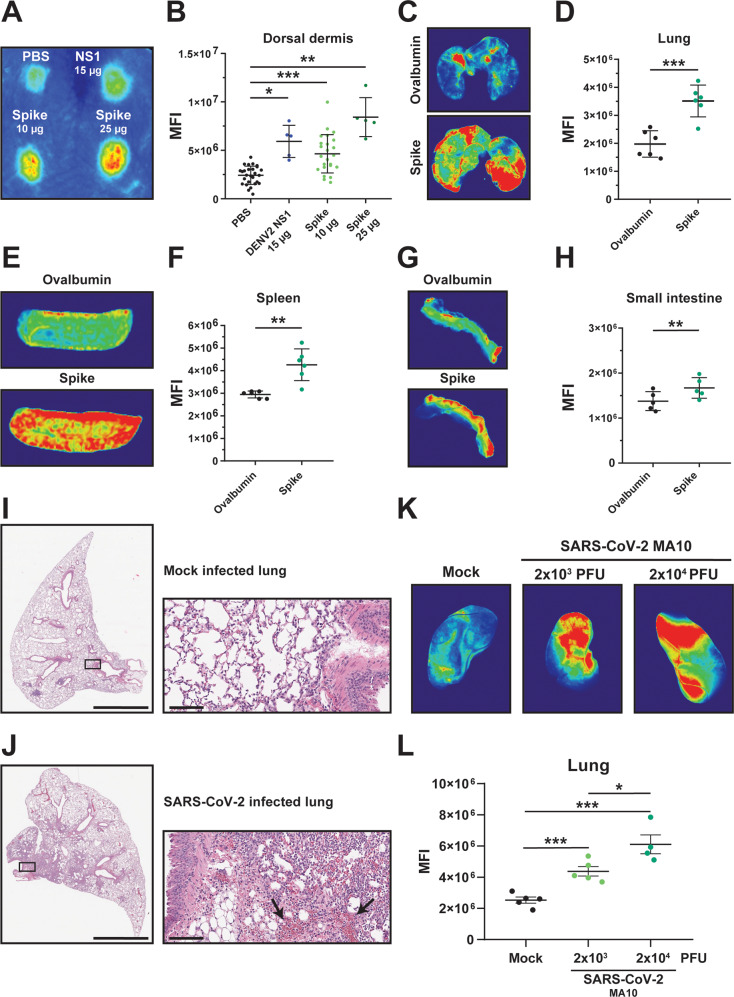
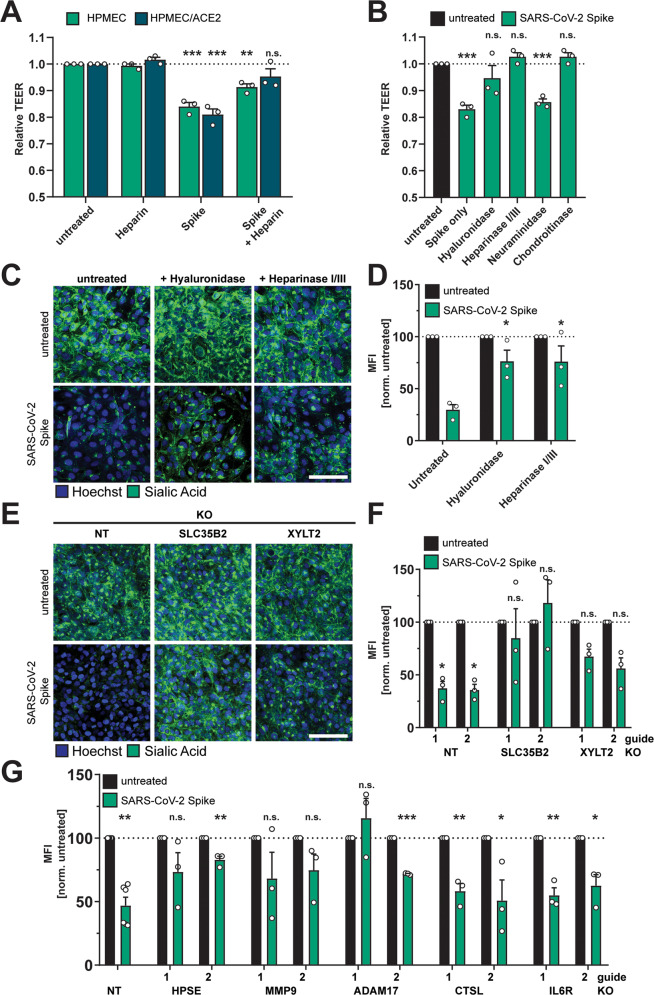
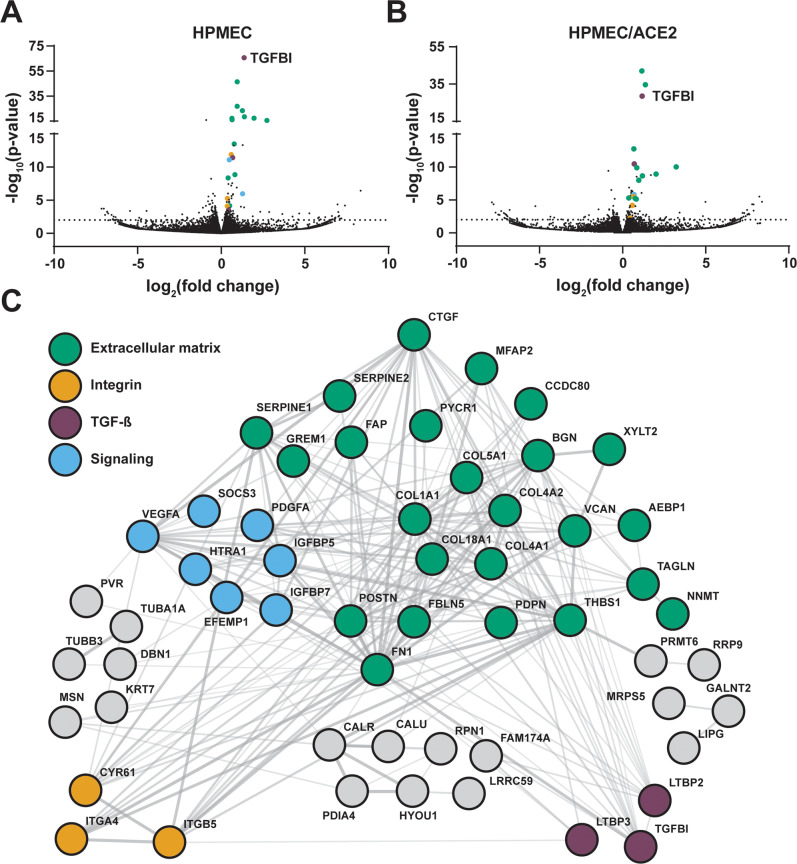
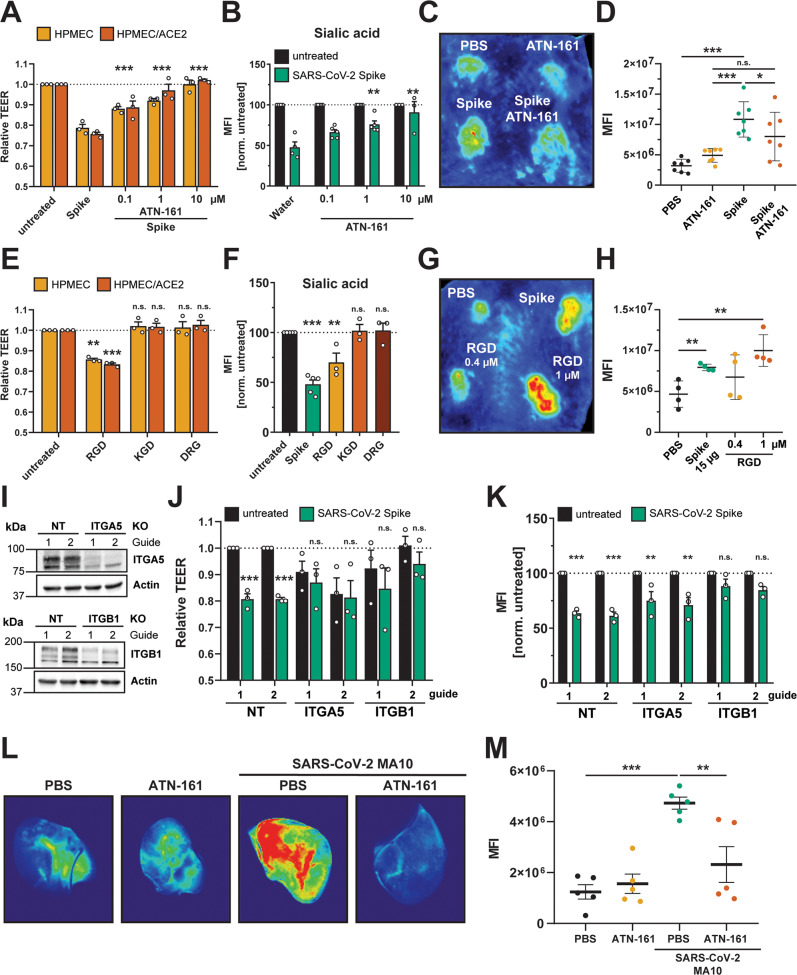
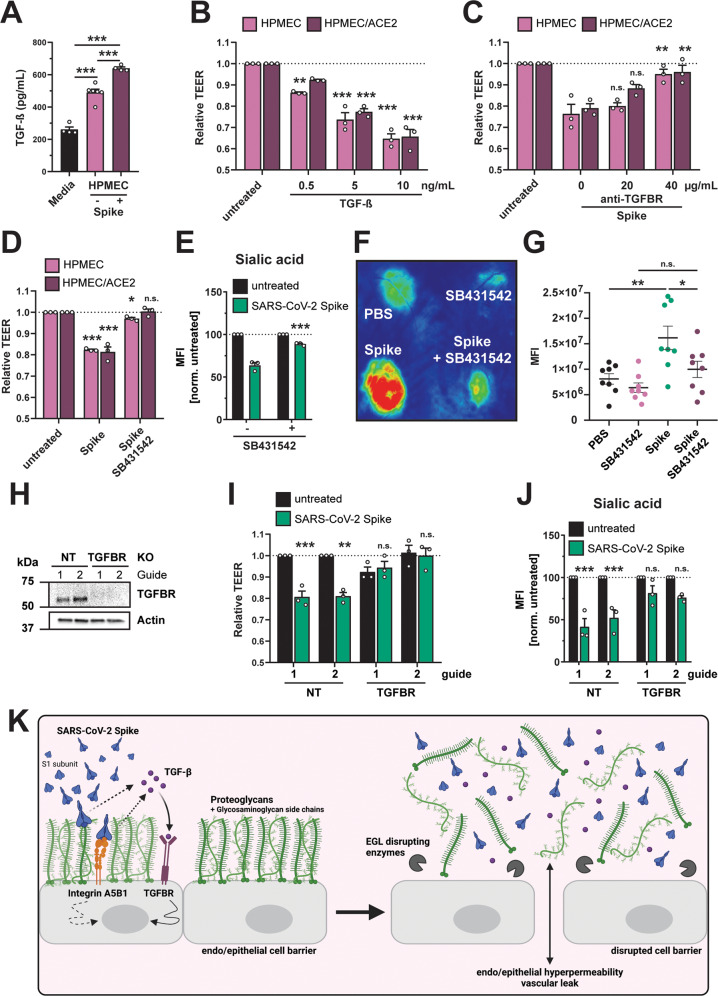
Severe COVID-19 is associated with epithelial and endothelial barrier dysfunction within the lung as well as in distal organs. While it is appreciated that an exaggerated inflammatory response is associated with barrier dysfunction, the triggers of vascular leak are unclear. Here, we report that cell-intrinsic interactions between the Spike (S) glycoprotein of SARS-CoV-2 and epithelial/endothelial cells are sufficient to induce barrier dysfunction in vitro and vascular leak in vivo, independently of viral replication and the ACE2 receptor. We identify an S-triggered transcriptional response associated with extracellular matrix reorganization and TGF-β signaling. Using genetic knockouts and specific inhibitors, we demonstrate that glycosaminoglycans, integrins, and the TGF-β signaling axis are required for S-mediated barrier dysfunction. Notably, we show that SARS-CoV-2 infection caused leak in vivo, which was reduced by inhibiting integrins. Our findings offer mechanistic insight into SARS-CoV-2-triggered vascular leak, providing a starting point for development of therapies targeting COVID-19.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
SARS-CoV-2 Spike triggers barrier dysfunction and vascular leak via integrins and TGF-β signaling.bioRxiv [Preprint]. 2021 Dec 13:2021.12.10.472112. doi: 10.1101/2021.12.10.472112. bioRxiv. 2021. Update in: Nat Commun. 2022 Dec 9;13(1):7630. doi: 10.1038/s41467-022-34910-5. PMID: 34931188 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
