

Obesity is associated with myelin oligodendrocyte glycoprotein antibody-associated disease in acute optic neuritis
- PMID: 36494385
- PMCID: PMC9734097
- DOI: 10.1038/s41598-022-21592-8
Obesity is associated with myelin oligodendrocyte glycoprotein antibody-associated disease in acute optic neuritis
Erratum in
-
Author Correction: Obesity is associated with myelin oligodendrocyte glycoprotein antibody-associated disease in acute optic neuritis.Sci Rep. 2023 Feb 20;13(1):2944. doi: 10.1038/s41598-023-30115-y. Sci Rep. 2023. PMID: 36807557 Free PMC article. No abstract available.
Abstract
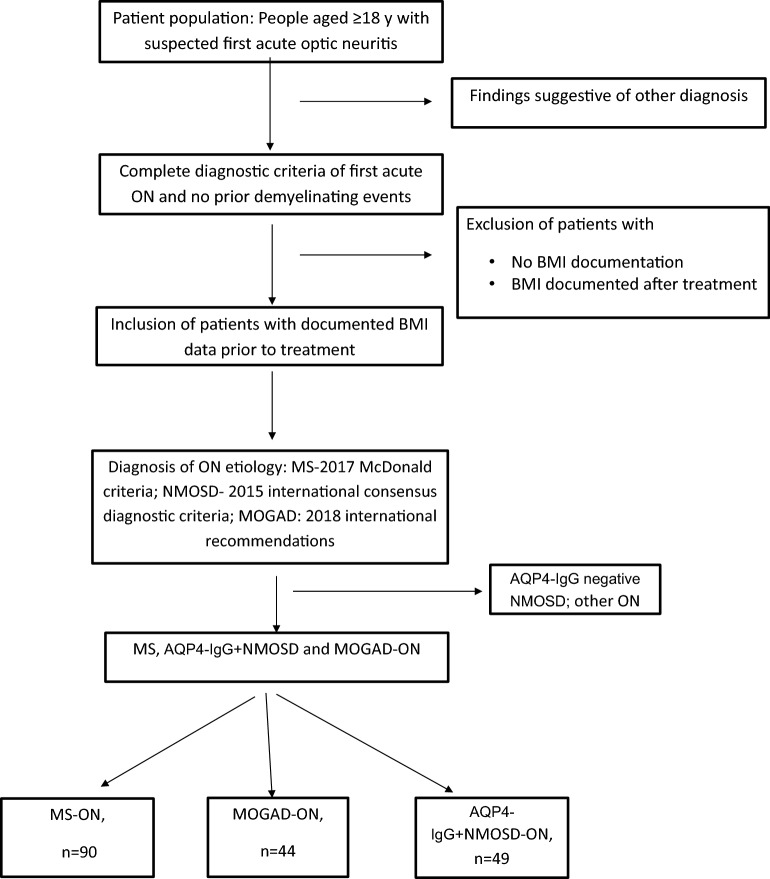
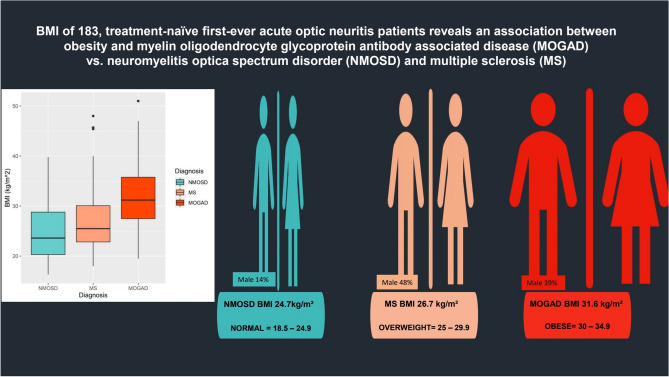
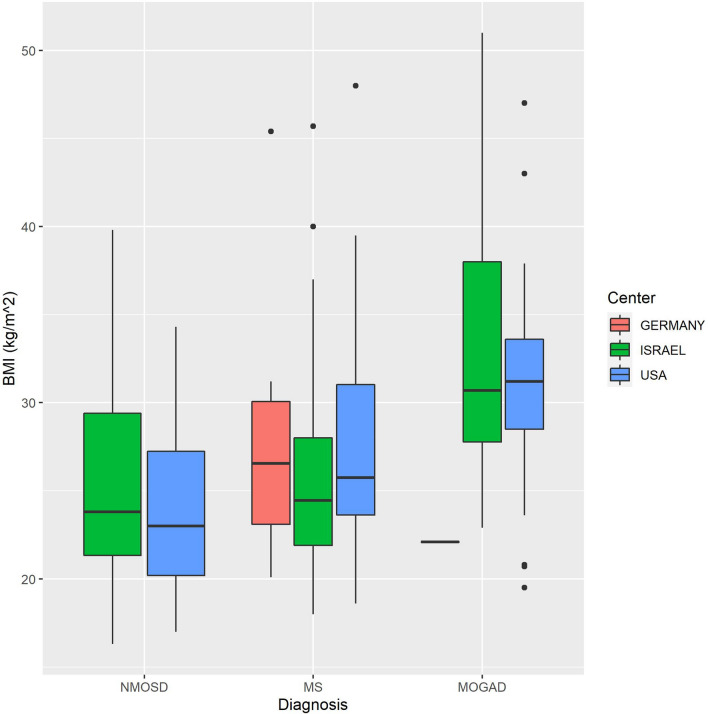
Optic neuritis (ON) is a frequent presentation at onset of multiple sclerosis (MS), neuromyelitis optica spectrum disorder (NMOSD), and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD). The pathophysiology underlying these diseases, especially MOGAD, is still being elucidated. While obesity has been reported to potentially be a risk factor for MS, this has not been explored in NMOSD or MOGAD. We aimed to investigate a possible association between obesity (body mass index [BMI] > 30 kg/m2) in patients with MOGAD, aquaporin 4-IgG positive NMOSD (AQP4-IgG+ NMOSD) or MS. In this multicenter non-interventional retrospective study, data was collected from patients with a first ever demyelinating attack of ON subsequently diagnosed with MOGAD (n = 44), AQP4-IgG+ NMOSD (n = 49) or MS (n = 90) between 2005 and 2020. The following data was collected: age, sex, ethnicity, BMI (documented before corticosteroid treatment), and the ON etiology after diagnostic work-up. A mixed model analysis was performed to assess the potential of obesity or BMI to predict MOGAD-ON, and to distinguish MOGAD-ON from AQP4-IgG+ NMOSD-ON and MS-ON. Main outcome measures included BMI in patients with acute ON and subsequent diagnosis of MOGAD, AQP4-IgG+ NMOSD or MS. A higher BMI was significantly associated with a diagnosis of MOGAD-ON (p < 0.001); in MOGAD patients the mean BMI was 31.6 kg/m2 (standard deviation (SD) 7.2), while the mean BMI was 24.7 kg/m2 (SD 5.3) in AQP4-IgG+ NMOSD patients, and 26.9 kg/m2 (SD 6.2) in MS patients. Mixed-effects multinomial logistic regression, adjusted for age and sex, with obesity as a binary variable, revealed that obesity was associated with a higher odds ratio (OR) of a subsequent MOGAD diagnosis (OR 5.466, 95% CI [2.039, 14.650], p = 0.001) in contradistinction with AQP4-IgG+ NMOSD. This study suggests an association between obesity and MOGAD. Our findings require further exploration, but could have significant pathophysiologic implications if confirmed in larger prospective studies.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
