

Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors
- PMID: 36494601
- PMCID: PMC9734185
- DOI: 10.1038/s41698-022-00334-z
Comprehensive pan-cancer genomic landscape of KRAS altered cancers and real-world outcomes in solid tumors
Abstract
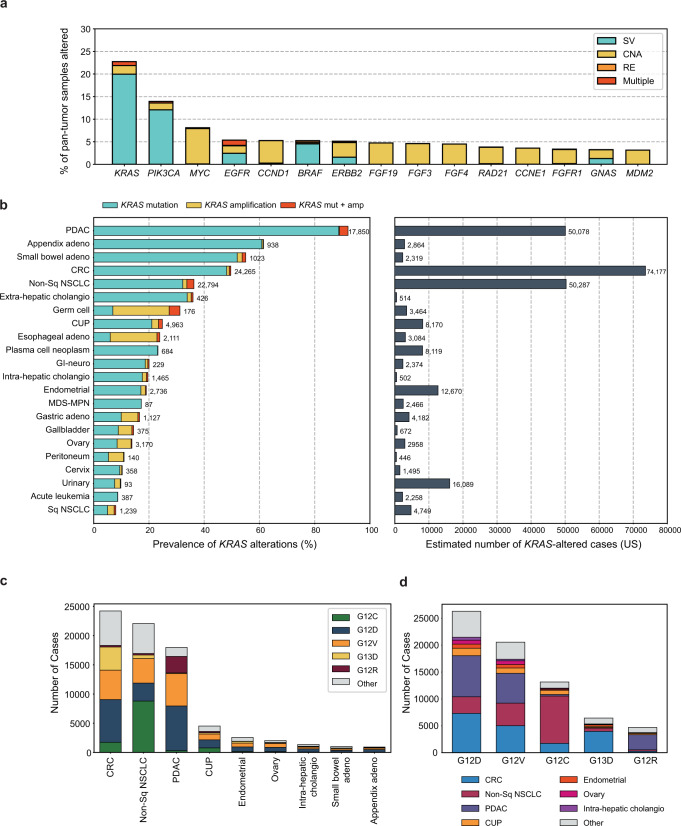
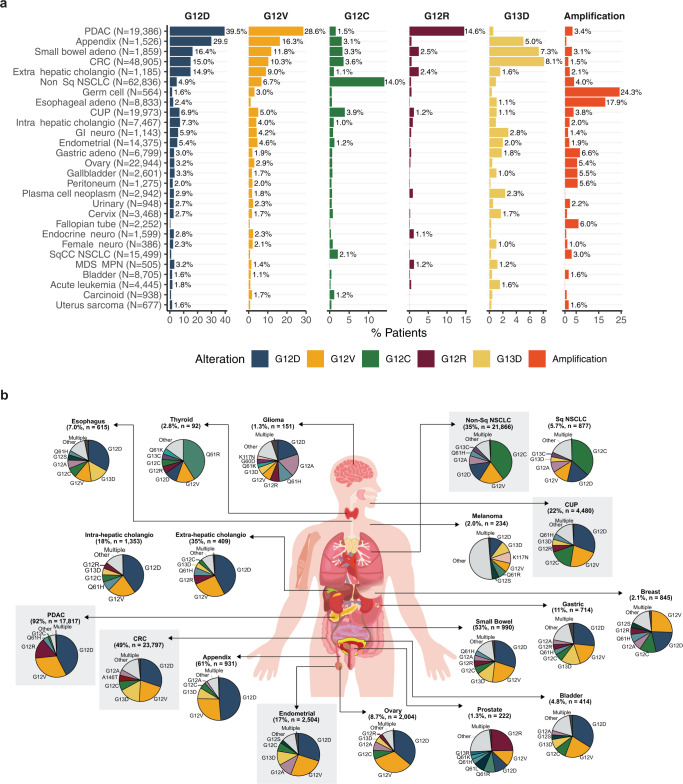
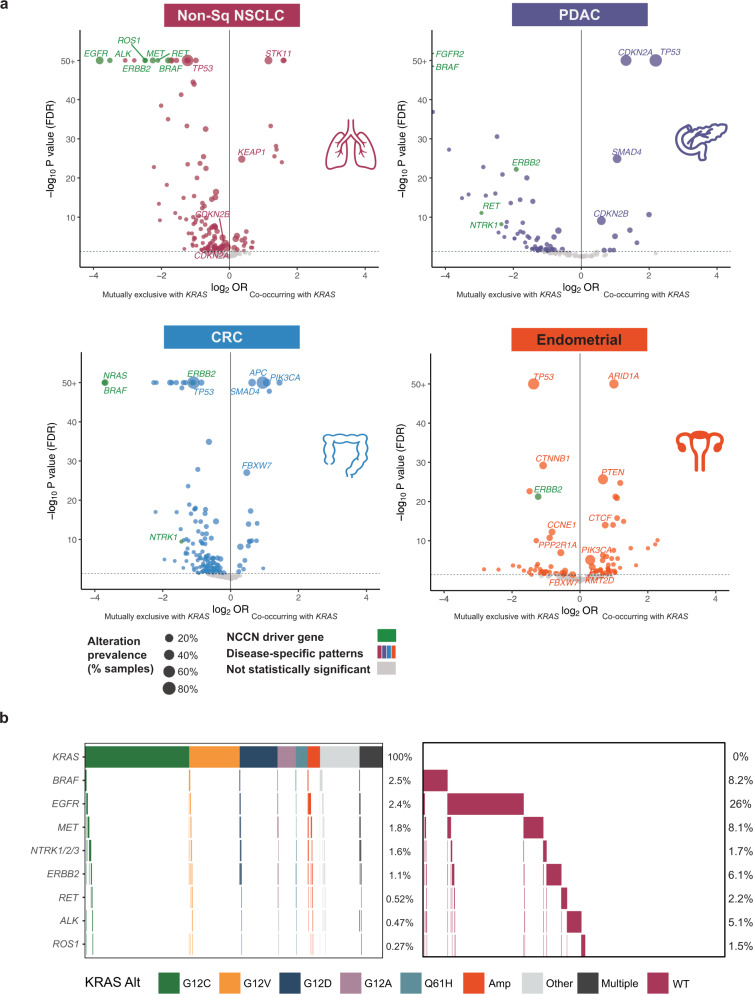
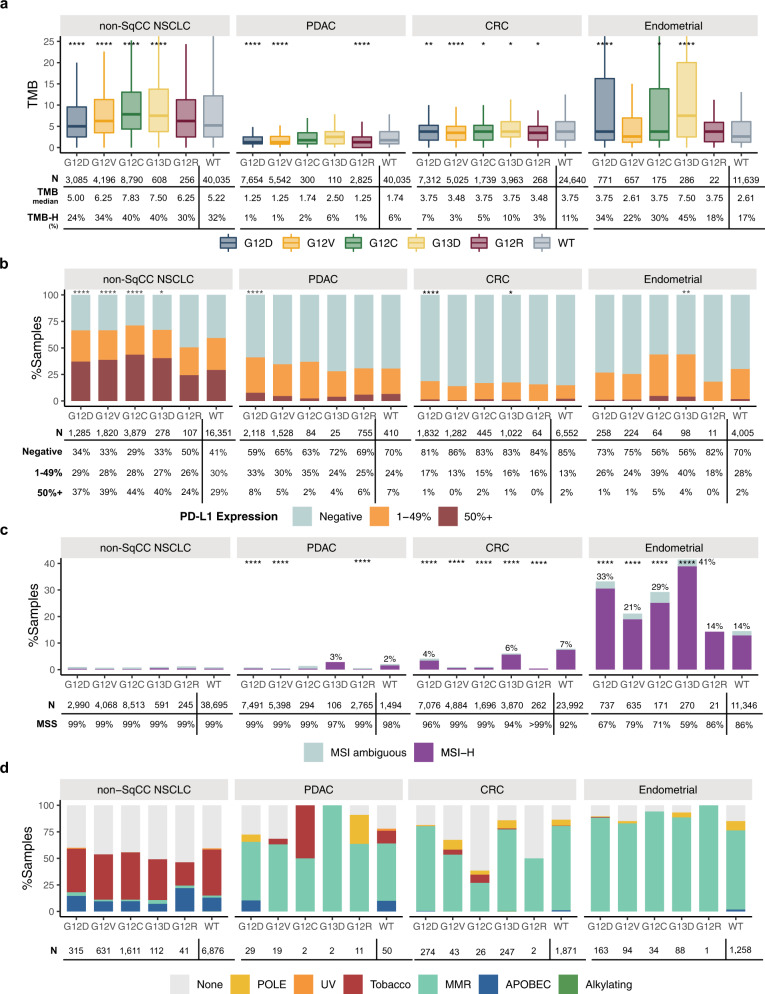
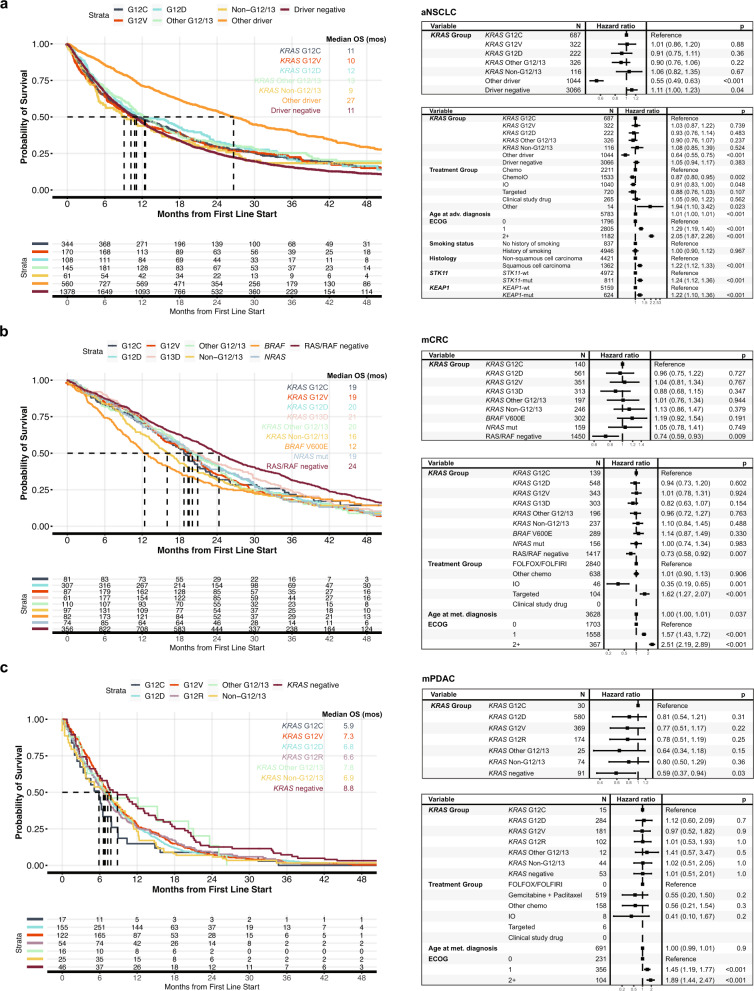
Recent clinical development of KRAS inhibitors has heightened interest in the genomic landscape of KRAS-altered cancers. We performed a pan-cancer analysis of KRAS-altered samples from 426,706 adult patients with solid or hematologic malignancies using comprehensive genomic profiling; additional analyses included 62,369 liquid biopsy and 7241 pediatric samples. 23% of adult pan-cancer samples had KRAS alterations; 88% were mutations, most commonly G12D/G12V/G12C/G13D/G12R, and prevalence was similar in liquid biopsies. Co-alteration landscapes were largely similar across KRAS mutations but distinct from KRAS wild-type, though differences were observed in some tumor types for tumor mutational burden, PD-L1 expression, microsatellite instability, and other mutational signatures. Prognosis of KRAS-mutant versus other genomic cohorts of lung, pancreatic, and colorectal cancer were assessed using a real-world clinicogenomic database. As specific KRAS inhibitors and combination therapeutic strategies are being developed, genomic profiling to understand co-alterations and other biomarkers that may modulate response to targeted or immunotherapies will be imperative.
© 2022. The Author(s).
Conflict of interest statement
J.K.L., S.S., A.B.S., R.M., D.F., O.G., J.S.R., G.M.F., M.M., G.R.O., P.S.H., and E.S.S. are employees of Foundation Medicine Inc, a wholly owned subsidiary of Roche, and have stock ownership in Roche. J.S.R. is consultant and stock owner in Celsius TX and Tango Tx. S.H.I.O. has received honorarium from Pfizer, Roche/Genentech, Takeda/ARIAD, Astra Zeneca, Daiichi Sankyo, BeiGene, Lilly, Caris Life Sciences Inc, has stock ownership in Turning Point Therapeutics and Elevation Oncology, and has been a member of scientific advisory board for Elevation Oncology. M.N. is on the advisory board for AstraZeneca, Daiichi Sankyo, Takeda, Novartis, EMD Serono, Janssen, Pfizer, Eli Lilly, and Company and Genentech; consultant for Caris Life Sciences (virtual tumor board); speaker for Blueprint Medicines and Takeda; and reports travel support from AnHeart Therapeutics. P.N., J.L.S., X.Y., and Z.S. are employees of Genentech, Inc. and have equity in Roche.
Figures
References
-
- Parada, L. F., Tabin, C. J., Shih, C. & Weinberg, R. A. Human EJ bladder carcinoma oncogene is homologue of Harvey sarcoma virus ras gene. Nature10.1038/297474a0 (1982). - PubMed
-
- Santos, E., Tronick, S. R., Aaronson, S. A., Pulciani, S. & Barbacid, M. T24 human bladder carcinoma oncogene is an activated form of the normal human homologue of BALB- and Harvey-MSV transforming genes. Nature10.1038/298343a0 (1982). - PubMed
-
- Taparowsky, E. et al. Activation of the T24 bladder carcinoma transforming gene is linked to a single amino acid change. Nature10.1038/300762a0 (1982). - PubMed
-
- Capon, D. J. et al. Activation of Ki-ras2 gene in human colon and lung carcinomas by two different point mutations. Nature10.1038/304507a0 (1983). - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
