

Current concepts in acromioclavicular joint (AC) instability - a proposed treatment algorithm for acute and chronic AC-joint surgery
- PMID: 36494652
- PMCID: PMC9733089
- DOI: 10.1186/s12891-022-05935-0
Current concepts in acromioclavicular joint (AC) instability - a proposed treatment algorithm for acute and chronic AC-joint surgery
Abstract
Background: There exists a vast number of surgical treatment options for acromioclavicular (AC) joint injuries, and the current literature has yet to determine an equivocally superior treatment. AC joint repair has a long history and dates back to the beginning of the twentieth century.
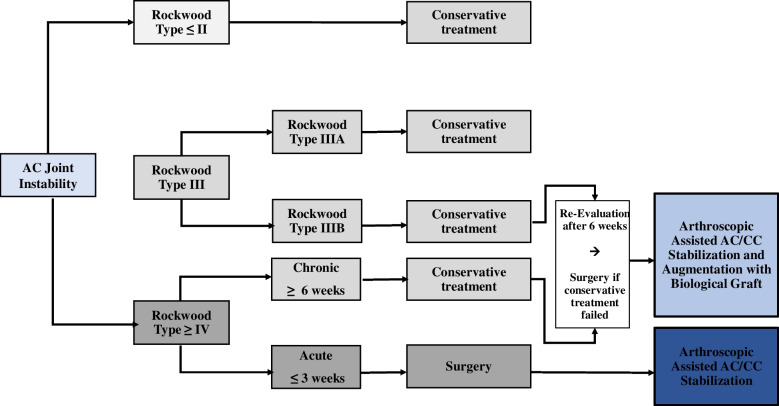
Main body: Since then, over 150 different techniques have been described, covering open and closed techniques. Low grade injuries such as Type I-II according to the modified Rockwood classification should be treated conservatively, while high-grade injuries (types IV-VI) may be indicated for operative treatment. However, controversy exists if operative treatment is superior to nonoperative treatment, especially in grade III injuries, as functional impairment due to scapular dyskinesia or chronic pain remains concerning following non-operative treatment. Patients with a stable AC joint without overriding of the clavicle and without significant scapular dysfunction (Type IIIA) may benefit from non-interventional approaches, in contrast to patients with overriding of the clavicle and therapy-resistant scapular dysfunction (Type IIIB). If these patients are considered non-responders to a conservative approach, an anatomic AC joint reconstruction using a hybrid technique should be considered. In chronic AC joint injuries, surgery is indicated after failed nonoperative treatment of 3 to 6 months. Anatomic AC joint reconstruction techniques along with biologic augmentation (e.g. Hybrid techniques, suture fixation) should be considered for chronic high-grade instabilities, accounting for the lack of intrinsic healing and scar-forming potential of the ligamentous tissue in the chronic setting. However, complication and clinical failure rates remain high, which may be a result of technical failures or persistent horizontal and rotational instability.
Conclusion: Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint.
Keywords: AC joint; Acromioclavicular joint; Acromioclavicular joint reconstruction; Anatomic acromioclavicular joint reconstruction; Horizontal instability; Vertical instability.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Beitzel K, Mazzocca AD, Bak K, Itoi E, Kibler WB, Mirzayan R, Imhoff AB, Calvo E, Arce G, Shea K. ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014;30(2):271–278. doi: 10.1016/j.arthro.2013.11.005. - DOI - PubMed
-
- Gowd AK, Liu JN, Cabarcas BC, Cvetanovich GL, Garcia GH, Manderle BJ, Verma NN. Current concepts in the operative Management of Acromioclavicular Dislocations: a systematic review and Meta-analysis of operative techniques. Am J Sports Med. 2019;47(11):2745–2758. doi: 10.1177/0363546518795147. - DOI - PubMed
-
- Aliberti GM, Kraeutler MJ, Trojan JD, Mulcahey MK. Horizontal instability of the acromioclavicular joint: a systematic review. Am J Sports Med. 2019;363546519831013. - PubMed
-
- Moatshe G, Kruckeberg BM, Chahla J, Godin JA, Cinque ME, Provencher MT, LaPrade RF. Acromioclavicular and Coracoclavicular ligament reconstruction for acromioclavicular joint instability: a systematic review of clinical and radiographic outcomes. Arthroscopy. 2018;34(6):1979–1995 e1978. doi: 10.1016/j.arthro.2018.01.016. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
